Sohail Shaikh1, Rajshree Dayanand Katke2, Soham Dilip Raut1
From the Department of Surgery1 and Department of Obstetrics & Gynecology2, Grant Government Medical College & Sir J. J. Group of Hospitals, Mumbai, Maharashtra, India.
Corresponding Author:
Dr. Rajshree Dayanand Katke
Email: drrajshrikatke@gmail.com
Abstract
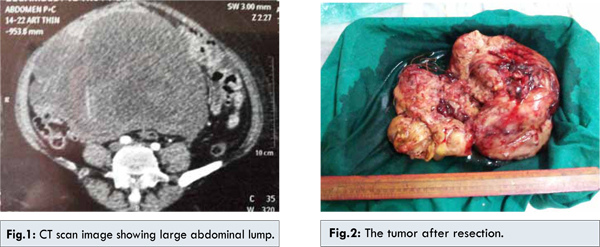
Spindle cell sarcoma is a rare tumor that arises most commonly from the peripheral and deep soft tissues. It can present as a large abdominal mass. We report the case of a 65 year old female who presented with abdominal distention. CT scan showed a mass occupying the whole of the abdomen and pelvis. Exploration of abdomen revealed a jelly like mass about 19.5x16x13 cm in size. Debulking surgery was done and on histopathology and immunochemistry a high grade spindle cell carcinoma was confirmed.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffe4d805000000f002000001000500 6go6ckt5b5idvals|336 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Spindle cell sarcoma is a type of connective tissue cancer in which the cells are spindle-shaped when examined on microscopy. The tumors generally begin in nerve sheath, layers of connective tissue such as that under the skin, between muscles, and surrounding organs, mesocolon, and will generally start as a small lump with inflammation that grows. Spindle cell tumors are low grade fibromyxoid soft tissue sarcoma and microscopic appearance with features of both mesenchymal and neuroendocrine differentiation. Cytogenetic studies of spindle cell tumor show two cell lines containing balanced translocation between chromosomes 7 and 16 [1]. A small group of both low grade fibromyxoid soft tissue sarcoma and hyalinizing spindle tumor (HSCT) shows areas of increased cellularity and atypia which are grouped as intermediate to high grade sarcoma [2]. A rare case of spindle cell carcinoma is documented in the esophagus [3]. These tumors rarely metastasize, but pulmonary metastases are documented [4,5].
Case Report
A case of 65 year old female, housewife, presented through the outpatient department with one month history of abdominal swelling and distention, weight loss, intermittent constipation and dysuria. Her vitals were within normal limits. On examination, abdomen was distended with everted umbilicus, dilated veins on left lower quadrant of abdomen with a hard non-tender mass almost occupying the whole of the abdomen arising from pelvis reaching up to just 5 cm below xiphisternum with smooth surface. Patient was previously operated for total abdominal hysterectomy with bilateral salpingoophorectomy, seven years ago for ovarian cancer.
CT scan report was suggestive of 19.5x16.3x13 cm well defined, heterogeneously enhancing mass lesion with necrotic areas in the midline arising from the pelvis and extending up to L3 vertebral body. The mass was compressing the bladder though the fat planes were maintained. The mass was reported most likely to be a neoplastic lesion [Fig.1]. Midline exploratory laparotomy showed a jelly like mass in the abdominal cavity and pelvis reaching up to the base of pelvis. The mass was approximately 20x15 cm in size, smooth in surface and rounded in shape [Fig.2]. Mass was separated from the surrounding structures and excised. Weight of the mass was 4.5 kg, measured after the surgery. Postoperative follow-up in the ward was uneventful and patient was transfused for the compensating the blood loss of about 700 ml during the surgery.
Histopathology report was suggestive of high grade spindle cell sarcoma [Fig.3]. Several foci of tumor necrosis. nuclear pleomorphism and mitotic activity were conspicuous. On immunohistochemistry, tumor cells were positive for S-100 with negative Desmin and SMA. Thus possibility of smooth cell differentiation was excluded and possibility of malignant nerve sheath tumor favored. No ovarian parenchyma was recognized. Patient was then referred to oncology for radiotherapy.
Discussion
Spindle cell sarcoma is a type of connective tissue cancer in which the cells are spindle-shaped when examined microscopically Spindle cell sarcoma is a rare cause of large abdominal mass [6]. Cytological diagnosis of spindle cell tumor is difficult as compared to other soft tissue tumors [7]. These tumors generally begin in layers of connective tissue such as that under the skin, between muscles, and surrounding organs, and will generally start as a small lump that grows gradually. At first the lump is self-contained as the tumor exists in earlier stages, and will not necessarily expand beyond its encapsulated form. However, it may develop malignant processes that can only be detected through microscopic examination. As such, at this level the tumor is usually treated by excision that includes wide margins through healthy-looking tissue, followed by thorough biopsy and additional excision if necessary. In high grade lesions, prognosis is grim and chemotherapy and radiation are the only methods of controlling the cancer.
Spindle cell sarcoma can develop for a variety of reasons, including genetic predisposition but it also may be caused by a combination of other factors including injury and inflammation in patients that are already thought to be predisposed to such tumors. Spindle cells are a naturally occurring part of the body’s response to injury. In response to an injury, infection, or other immune response the connective tissues will begin dividing to heal the affected area, and if the tissue is predisposed to spindle cell cancer the high cellular turnover may result in a few becoming cancerous and forming a tumor.
Spindle cell tumors are usually diagnosed on histopathology based on picture comprising of elongated spindle cells arranged in interlacing fascicles and bundles with herring bone pattern at places. These bundles intersect each other at wide angles at places showing storiform pattern with eosinophilic cytoplasm and cigar shaped nuclei. Occasionally ghost cells in the center and multinucleated giant cell may present, grading is suggested in soft tissue sarcoma in order to improve the management, prognosis and to prevent the recurrence, based on nuclear atypia, nuclear overlap, mitotic figures, and necrosis these tumors are given grades [8,9]. Treatment of spindle cell tumor is its complete excision [10]. Radiotherapy has minimal role and the tumor tends to recur. In our case, spindle cell sarcoma of nerve sheath occurring in the abdomen was a rare case. The size upto which it progressed posed a great challenge during surgery as the tumor mass was jelly like and friable. The tumor had to be meticulously dissected away from the small bowel at the same time achieving adequate hemostasis.
References
- Reid R, de Silva MV, Paterson L, Ryan E, Fisher C. Low grade fibromyxoid sarcoma and hyalinizing spindle cell tumor with giant rosettes share a common t(7;16)(q 34;p11) translocation. Am J Surg Pathol 2003;27:1229-1236.
- Yang S, Liu C, Chai C, Chien S, Wang C. Hyalinizing spindle cell tumor with giant rosettes: a case report. Kaohsiung J Med Sci 2009;25:583-586.
- Yakoob J, Abbas Z, Jaffery W, Azad SN. Esophageal polypoidal mass: presentation of an uncommon pleomorphic carcinoma. J Pak Med Assoc 2009;59:756-759.
- O Sulvian MJ, Sirgi KE, Dehner LP. Low grade fibrosarcoma (Hyalinizing spindle cell tumour with giant rosettes) with pulmonary metastases at presentation: case report and review of the literature. Intern J Surg Pathol 2002;10:211-216.
- Loya A, Prayaga AK, Arora A, Sundaram C, Rao SI, Uppin SG, et al. Lymph node metastasis of soft tissue tumours: a cytomorphologic study. Acta Cytol 2007;51:153-160.
- Bills V, Iqbal R, Haqqani M, Clague JE. Spindle cell sarcoma: a rare cause of a large abdominal mass. Age Ageing 2005;34:88-89.
- Prayaga A. Cytology of soft tissue tumours: Malignant spindle cell tumours. J Cytol 2008; 25:87-88.
- Mathur S, Kapila K, Verma K. Accuracy of cytologic grading of spindle cell sarcomas. Diagn Cytopathol 2003;29:79-83.
- Jones C, Liu K, Hirschowitz S, Klipfel N, Layfield LJ. Concordance of histopathologic and cytologic grading in musculoskeletal sarcomas; Can grade obtained from analysis of fine needle aspirates serve as the basis for the therapeutic decisions? Cancer 2002;96:83-91.
- Fras AP, Grazio SAF. Hyalinizing spindle cell tumour with giant rosettes of the broad ligament. Gynecologic Oncol 2001;83:405-408.
|