Pranita Medhi, Swagata Dowerah, Mahak Sarma, Farzana Z Ahmed
Department of Pathology and Obstretics & Gynaecology, Assam Medical College, Dibrugarh, Assam, India.
Corresponding Author:
Dr. Pranita Medhi
Email: pranita_medhi@yahoo.co.in
Abstract
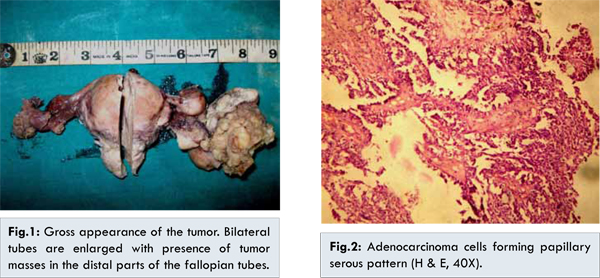
Introduction: Primary carcinoma of the fallopian tube is one of the rarest malignant tumors, accounting for 0.3%-0.8% of all gynecologic malignancies. Case Report: A 57 year old postmenopausal female presented with abdominal pain and serosanguinous vaginal discharge of six months duration. A vague mass was palpable in the lower abdomen. Transvaginal ultrasonography revealed bilateral tubo-ovarian masses. Patient underwent abdominal hysterectomy with bilateral salpingo-oophorectomy. On gross examination, uterus, cervix and ovaries were normal. Left and right fallopian tubes were enlarged with irregular greyish white masses in the ampullary region, measuring 6x5x3 cms and 3x2x2 cms respectively. Cut surface was solid cystic with friable greyish white papillary growths on both sides. Microscopy revealed adenocarcinomatous cells showing a papillary growth pattern. A diagnosis of bilateral primary papillary serous adenocarcinoma was made. Conclusion: This case is reported for its rare occurrence.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa8ad07000000fd03000001000100 6go6ckt5b5idvals|491 6go6ckt5b5|2000F757Tab_Articles|Fulltext Case Report
A 57 year old postmenopausal female presented in the gynaecology outpatient department with intermittent abdominal pain and serosanguinous vaginal discharge of six months duration. A vague mass was palpable in the lower abdomen. Per vaginal examination was normal. Routine investigations and chest X-ray were within normal limit. Transvaginal ultrasonography revealed bilateral tubo-ovarian masses only without any other significant findings. Ovarian tumor was suspected and patient underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy. On gross examination, uterus, cervix and both ovaries were normal. Left and right fallopian tubes were enlarged with irregular greyish white masses in the ampullary region, measuring 6x5x3 cms and 3x2x2 cms respectively [Fig.1]. Cut surface was solid cystic with friable greyish white papillary growths on both sides. Microscopic examination revealed adenocarcinomatous cells showing a papillary growth pattern and mitotic figures [Fig.2]. Lymph nodes and omentum submitted were free from malignant cells. A diagnosis of bilateral primary papillary serous adenocarcinoma was made based on the above findings. The tumor was staged as FIGO stage IB. Post-operatively patient did not received any adjuvant chemotherapy. Patient has been followed up at 6 months and one year post surgery and is doing well.
Fallopian tube cancer is the least common of gynaecological malignancies. It was first described by Renaud in 1847 [ 4]. Carcinoma of the fallopian tube is generally recognized as a disease of menopausal women [ 5]. Latzko’s triad of symptoms, which consist of an intermittent, profuse, serosanguinous vaginal discharge, a colicky pain which is relieved by discharge, and abdominal or pelvic masses, has been reported in 15% of the cases [ 6]. Although the classic triad of symptoms is said to be pathognomonic, the correct preoperative diagnosis is made in only 4% of the cases [ 7]. Often, the diagnosis is mistaken for ovarian cancer or a tubo-ovarian mass as was seen in our case. The diagnosis of primary fallopian tube carcinoma is usually first made by a pathologist during a histopathological examination.
Bilateral involvement is reported to occur in 10%-20% of patients but in one series, the figure is only 3% [ 8]. For diagnosing primary tubal carcinoma, both the ovaries and the uterus should appear normal on gross examination. The tubes, at least in the distal portion should be grossly abnormal. The fimbriated ends may be dilated and occluded resembling chronic salpingitis [ 9].
The most common histological types of primary fallopian tube carcinoma are serous, endometrioid, mixed, undifferentiated, clear cell, transitional, and mucinous. The serous and the endometrioid types are more commonly seen. It is difficult to differentiate primary fallopian tube carcinoma from epithelial ovarian carcinoma. The patients should meet at least one of the following criteria for the diagnosis of primary fallopian tube carcinoma [ 11]. (a) The main tumour is in the tube and it arises from the endosalpinx; (b) Histologically, the pattern reproduces the epithelium of the mucosa and it often shows a papillary pattern; (c) If the wall is involved, the transition between the benign and the malignant epithelium should be demonstrable and (d) The ovaries and the endometrium are either normal or they may contain less tumour than that which is there in the tube.
CA-125 is also a useful early and a sensitive marker for the tumor progression during the follow-up [ 12]. The most important prognostic factor in fallopian carcinoma is stage of disease at laparotomy. The 5-year survival of fallopian tube carcinoma (stage I and II) is poorer at 50.8% than that of ovarian cancer at 77.5% [ 13].
Conclusion
This case is reported for its rare occurrence. We would also like to emphasise the fact in a postmenopausal woman with tubo-ovarian mass, a diagnosis of fallopian tube carcinoma needs to be kept in mind.
References
- Nordin AJ. Primary carcinoma of the fallopian tube: a 20-year literature review. Obstet Gynecol Surv. 1994;49:349-361.
- Markman M, Zaino RJ, Fleming PA, Barakat RR. Carcinoma of the fallopian tube. In: Hoskins WJ PCYR (editor). Principles and Practice of Gynecologic Oncology. Philadelphia: Lippincott Williams and Wilkins; 2000. pp. 1099-1112.
- Honoré LH. Pathology of the fallopian tube and broad ligament. In: Fox H, Wells M. Haines and Taylor Obstetrical and Gynecologic Pathology. 5th. New York: Churchill Livingstone; 2003. pp. 605-615.
- Lawson F, Lees C, Kelleher C. Primary cancer of the Fallopian tube. In: J IS, (editor). Progress in Obstetrics and Gynaecology. UK: Churchill Livingstone; 1996. pp. 393-401.
- Heintz AP, Odicino F, Maisonneuve P, Beller U, Benedet JL, Creasman WT, et al. Carcinoma of the fallopian tube. Int J Obstet Gynecol. 2003;83:119-133.
- Ajithkumar TV, Minimole AL, John MM, Ashokkumar OS. Primary fallopian tube carcinoma. Obstet Gynecol Surv. 2005;60:247-252.
- Riska A, Lemien A. Updating on primary fallopian tube carcinoma. Acta Obstet Gynecol Scand. 2007;86:1419-1426.
- Alvaredo-Cabrero I, Young RH, Vamvakakas EC, Scully RE. Carcinoma of the fallopian tube: a clinicopathological study of105 cases with observations on staging and prognostic factors. Gynecol Oncol. 1999;72:367-379.
- Saxena Bharti, Bansal MC, Gupta AR, Sharma Usha, Tanwar Rajendra Kumar, Mangal Kalpana. Fallopian tube carcinoma - A case report. J Obstet Gynecol India. 2007;57:81-82.
- Peters WA 3rd, Andersen WA, Hopkins MP, Kumar NB, Morley GW. Prognostic features of carcinoma of the fallopian tube. Obstet Gynecol. 1988: pp. 757-762.
- Hu CY, Taymor ML, Hertig AT. Primary carcinoma of the fallopian tube. Am J Obstet Gynecol. 1950;59:58-67.
- Niloff JM, Knapp RC, Schaetzl E, Reynolds C, Bast RC Jr. CA125 antigen levels in obstetric and gynecologic patients. Obstet Gynecol. 1984;64:703-707.
- Rosen AC, Sevelda P, Klein M, Graf AH, Lahousen M, Reiner A, et al. A comparative analysis of management and prognosis in Stage I and II fallopian tube carcinoma and epithelial ovarian cancer. Br J Cancer. 1994;69:577-579.
|