Introduction
Obturator hernia is a type of pelvic hernia in which a bowel segment protrudes through the obturator foramen adjacent to the obturator vessels and nerve. It occurs more frequently in patients with ascites, chronic constipation, chronic obstructive pulmonary disease and in thin, elderly multiparous women. The most common clinical symptom is strangulation combined with mechanical intestinal obstruction.
Obturator hernia is difficult to diagnose due to nonspecific symptoms, and most patients are diagnosed during surgery when they present with intestinal obstruction. Obturator hernias occur frequently in elderly patients with accompanying diseases, and therefore the morbidity and mortality rates are high. Currently, computed tomography, is widely used to diagnose obturator hernias before surgery in the early stages of the disease. The aim of this case report was to present the case, of a patient with mechanical intestinal obstruction who was diagnosed with obturator hernia using computed tomography.
Case Report
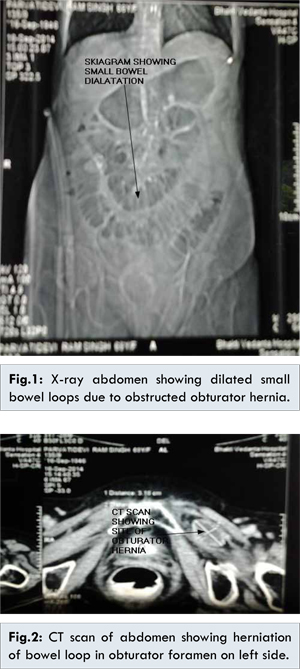
A 68 year female presented with pain abdomen and bilious vomiting since last 15 days. This was associated with abdominal distension and pain on medial aspects of thighs. She was admitted under physician as a case of acute gastroenteritis with acute renal failure. Ultrasound examination of abdomen showed some free fluid in abdomen. Physicians had ignored mild pain, projectile vomiting and failed to take surgical opinion in time. Upper gastrointestinal endoscopy showed some degree of reflux in lower end of oesophagus and antral gastritis. CT scan showed presence of small bowel dilatation with proximal ileal obstruction due to left sided obturator hernia [Fig.1]. CT scan also showed hernia sac contained a loop of proximal ileum in it and appeared viable but completely obstructed as seen by non-passage of contrast beyond site of obstruction [Fig.2]. There was no evidence of bowel perforation.
Detailed history and examination was suggestive of intestinal obstruction. Laparoscopy showed obstructed proximal ileal loop in obturator fossa. Ileal loop was released gently from obturator foramen. The obstructed segment had perforated due to prolonged obstruction leading to thinning of bowel. A lower abdomen transverse incision was taken for purpose of repair of hernia and closure of perforation. Perforation was closed with linear stapler and hernia was repaired in layers.
Discussion
Obturator hernias are notorious for diagnostic difficulty. Increasing speed of diagnosis through early CT imaging has been shown to reduce the morbidity and mortality associated with obturator hernias. Arnaud de Ronsil first described the obturator hernia in 1724 and Obre performed the first successful operation in 1851 [
1]. It is a rare condition with only 541 cases having been reported in the literature by 1980 [
2].
Obturator hernias are common in elderly female and post-pregnancy patients owing to the larger obturator canal, and increased laxity of the pelvic tissues [
3]. Upto 80% of patients with obturator hernias usually have symptoms of bowel obstruction, which is often partial due to a high proportion exhibiting Richter’s herniation [
4]. Obturator hernia sacs often compress or irritate the obturator nerve running in the canal, causing medial thigh pain such as the type exhibited in our case [
4].
Early diagnosis of obturator hernia can be made with CT of the abdomen and pelvis. It shows bowel herniating through the obturator foramen and lying between the pectineus and obturator [
7]. Abdominal, inguinal, retropubic, obturator, and laparoscopic approaches have all been described. The majority of published evidence favours the abdominal approach, utilizing a low midline incision. Simple closure of the hernial defect with interrupted sutures or placement of mesh are the preferred methods of herniorraphy as they are associated with the lowest complication rates [
4].
Both trans-abdominal and extra-peritoneal laparoscopic approaches have been described in the literature [
8]. Laparoscopic repair has been shown to produce less post-operative pain, fewer pulmonary complications and shorter hospital stays in such cases.
Conclusion
Obturator hernias carry significant morbidity and mortality rates, therefore rapid clinical and radiological assessment followed by early surgery is critical to successful treatment. Open approaches are well documented with good hernial defect repair rates. Laparoscopic repair may be appropriate in the classical patients.
References
- Bjork AKJ, Cahill DR. Obturator hernia. Surgery, Gynecology and Obstetrics. 1988;167:217-222.
- Ho YH, Goh HS. Obstructed obturator hernia in 90 year olds- a management dilemma. Annals of the Academy of Medicine. 1991;20(3):410-411.
- De Clerq L, Coenegrachts K, Feryn T, Van Couter A, Vandevoorde P, Verstraete K. An elderly woman with obstructed obturator hernia: a less common variety of external abdominal hernia. Journal Belge de Radiologie-Belgisch Tijdschrift voor Radiologi. 2010;93:302-304.
- Mantoo SK, Mak K, Tan TJ. Obturator hernia: diagnosis and treatment in the modern era. Singapore Medical Journal. 2009;50(9):866.
- Jamadar D, Jacobson J, Morag Y, Girish G, Ebrahim F, Gest T. Sonography of inguinal region hernias. American Journalism Review. 2006;187:185-190.
- Yokoyama Y, Yamaguchi A, Isogai M, Hori A, Kaneoka Y. Thirty-six cases of obturator hernia: Does computerized tomography contribute to postoperative outcome? World Journal of Surgery. 1999;23:2144-2147.
- Dundamadappa SK, Tsou IY, Goh JS. Clinics in diagnostic imaging. Singapore Medical Journal. 2006;47:88-94.
- Moreno-Egea A, La Calle MC, Torralba-Martinez JA. Obturator hernia as a cause of chronic pain after inguinal hernioplasty: elective management using tomography and ambulatory total extraperitoneally laparoscopy. Surgical Laparoscopy Endoscopy & Percutaneous Techniques. 2006;16:54-57.