Introduction
Cryptorchidism is the most common congenital genitourinary anomaly in men [
1]. It is a well-known risk factor for the testicular germ cell tumors (TGCTs). The risk of malignancy in an undescended testis is 10% with the highest risk in an intra-abdominal testis [
2]. We here present a case of an intra-abdominal testicular seminoma in middle aged man as an asymptomatic abdominal mass.
Case Report
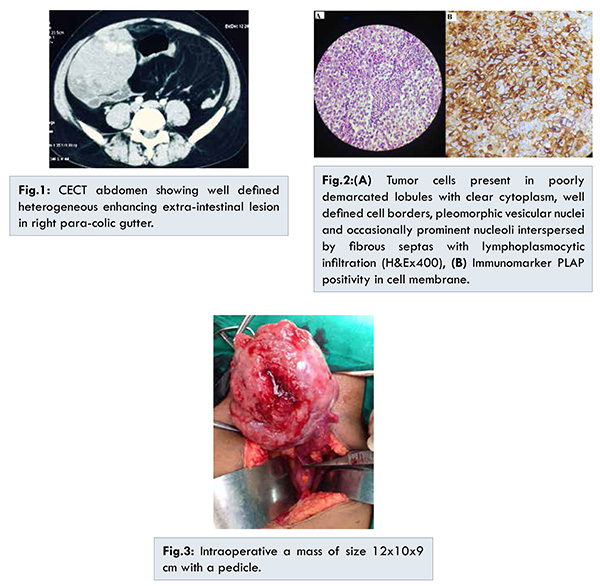
A 41-year fertile male was admitted with complaint of vague right abdominal pain for last one month. He had history of left orchidopexy in childhood. On clinical examination, there was an ill-defined mass in right lumbar region extending to the right iliac fossa. Only left testis was felt in scrotum with right hemiscrotum undeveloped. Contrast enhanced computerized tomography (CECT) abdomen showed a well-defined heterogeneous enhancing extra-intestinal lesion in right para-colic gutter of size 11x8x9 cms [Fig.1]. While image guided aspiration cytology reported it as malignant lesion with indeterminate histology, the core needle biopsy showed cells present in poorly demarketed lobules with clear cytoplasm, well defined cell borders, pleomorphic vesicular nuclei and occasionally prominent nucleoli interspersed by fibrous septas with lymphoplasmocytic infiltration which confirmed as seminoma [Fig.2(A)]. It was positive for PLAP, CK7 and negative for CK20, CD30, Desmin, LCA, S100 and CD138 with Ki-67 index 55% [Fig. 2(B)]. Among tumor markers, LDH was marginally raised and rest were within normal limits. Metastatic workup and other routine investigation were within normal limits. Patient underwent exploratory laparotomy where a solid mass of size 12x10x9 cm was found with a pedicle to the right internal inguinal ring with ascites [Fig.3]. The peritoneal fluid cytology was also positive for malignant germ cells. Final histology report confirmed it as seminoma with unremarkable capsule and epididymis. Patient than received chemotherapy and post-operative tumor markers were within normal limits.
The testis is an intra-abdominal organ during development which descends into the scrotal sac, usually between 28 to 32 weeks. It may get arrested anywhere along its tract (cryptorchidism) or may migrate into an abnormal position (ectopic testis) during descent. The most common sites of undescended testis are high scrotal (50%), canalicular (20%), and abdominal (10%) [
3]. The risk of cancer in undescended testis is 10% [
2].
Cryptorchidism is a main risk factor for TGCT. The incidence of carcinogenesis is 40 times higher in an undescended testis than in a normal scrotal testis. Furthermore, the malignant degeneration of an abdominal testis (5%) is four times more likely than an inguinal testis (1.25%) [
4]. The incidence curve of malignancy in undescended testes increases steeply after the onset of the puberty, usually peaks in the third or fourth decade of life [
1]. However, the cause of carcinogenesis is still an enigma. The most common clinical presentation in abdominal cryptorchid testis cancer is painless enlarging abdominal mass and occasionally with vague abdomen pain and secondary symptoms from effects of the mass [
5]. The rare presentations of the intra-abdominal germ cell tumors reported in literature are acute abdomen with intestinal perforation and haemorrhagic shock with tumor rupture [
6,
7].
Seminoma (90%) is the most common histology of tumors in undescended testis, particularly in the intra-abdominal testis [
8]. CT and MRI are the best imaging tool for the diagnosis [
9]. In an elderly male with nonspecific intra-abdominal mass, the differential diagnosis could be sarcoma, lymphoma or other malignancies. The laparoscopy is a minimal invasive procedure to diagnose and locate the intra-abdominal testis. The image guided core needle biopsy is the most valuable for histological diagnosis but has the risk of peritoneal seeding. The seminoma is PLAP and CK7 positive which helps in confirming the diagnosis [
10]. The germ cell tumors spread to retroperitoneal lymph nodes, except choriocarcinoma, which has early hematogenous spread. In case of intra-abdominal seminoma, the risk of peritoneal spread is high as in our case peritoneal fluid was positive for malignant germ cell. The excision of seminoma is the primary treatment irrespective of location and the adjuvant therapy is according to pathological stage. In present case it was seminoma stage IIIC and patient was given adjuvant chemotherapy. Although, there is 5%-20% risk of cancer in normal descended contralateral testis in cryptorchid patient, but there are no definitive guideline for the surveillance or management [
10].
Post-operative serum tumor markers has significance in both seminoma and non-seminoma germ cell tumors. Raised AFP, beta-HCG and LDH level is suggestive of advanced disease [
8]. The prognostic factors in seminoma are age of the patient, tumor size, lymphovascular invasion, mitotic count, necrosis, giant cells and lymphocytic infiltration.
Conclusion
The abdominal cryptorchid testis is rare and carries the highest risk of malignant transformation to seminoma among undescended testis variants. It usually presents with non-specific symptoms so complete systemic physical examination should not be neglected in an elderly patient with intra-abdominal mass. In developing country like ours, poor educational level of patient and inaccessibility of health care facilities leads to delayed presentation of the patient. However, awareness regarding undescended testis and its related complications must be increased at various levels by the parents, school medical officer and the patient himself.
References
- Alshyarba MH. A giant intra-abdominal testicular seminoma. Biomed Res. 2010;21(3):227-229.
- Cristián Palma C, Cristóbal B, Maccioni R. Seminoma in an adult cryptorchid testis (intra-abdominal): a case report. Actas Urol Esp. 2007;31(2):160-163.
- Dahnert W. Testicular tumor. In: Radiology review manual (5th ed). Williams and Wilkins; 2003:925.
- Whitaker RH. The undescended testis the risk of malignant degeneration. Monogr Paediatr 1981;12:104-108.
- Koh KB. Beware the undescended testis and abdominal mass. Aust N Z Surg. 1996;66:851-853.
- Watkins GL. Massive hemoperitoneum resulting from rupture of a seminoma in an undescended testicle. J Urol. 1970:103:447-448.
- Hutcheson JC, Khorasani R, Capelouto CC, Moore FD Jr, Silverman SG, Loughlin KR. Torsion of intraabdominal testicular tumors. A case report. Cancer. 1996:77:339-343.
- Woodward PJ. Seminoma in an undescended testis. Radiology. 2004;231:388-392.
- Bree RL, Hoang DT. Scrotal ultrasound. Radiol Clin North Am. 1996:6:1183-1205.
- Batata M, Chu F, Harris B, et al. Testicular cancer in cryptorchids. Cancer. 1982; 49:1023-1030.