Introduction
Infrahyoid muscles include superficially placed sternohyoid (SH) and omohyoid (OH) along with deeper sternothyroid and thyrohyoid. Omohyoid runs obliquely in lateral cervical region and consists of two bellies with an intermediate tendon. Variations in the infrahyoid muscles were identified as early as 19th century [
1]. Several authors have attempted to classify the anatomical variation that constitutes a muscle inserting from the clavicle into the hyoid bone. Loth classified it as cleidohyoid (CH) muscle by as early as 1912 [
2]. Others have described such muscle as cleidohyoideus accessorius muscle in the presence of intact omohyoid [
3,
4]. In such cases it is thought to be a variant of sternohyoid muscle. But here in this report presence of CH is reported with the absence of OH on the same side with no other abnormality. The question arises, whether it is a variant of OH or SH as both muscles have rare variants which have such attachment i.e. between clavicle and hyoid.
Case Report
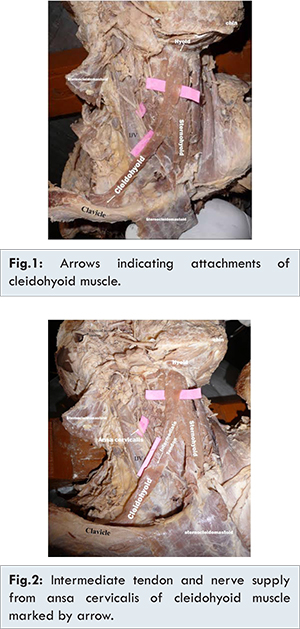
During routine dissection of male cadaver at the department of anatomy, Government medical college, Kota, on the right side the cadaver exhibited a normal sternothyroid, sternohyoid and thyrohyoid muscle. There was absence of omohyoid, instead a fourth atypical infrahyoid muscle was present on this side which originated from the clavicle and inserted on the hyoid bone. It was a flat, strap muscle 12 cm long and 2 cm wide. It had a fan shaped origin from posterior aspect of middle two third aspect of clavicle, passes upwards and forwards across the lower part of the neck. In the middle, similar to omohyoid, it presented with intermediate tendon. Thereafter it curved upwards got inserted to antero-lateral aspect of body of hyoid bone [Fig.1]. As there was no scapular attachment, this muscle was best described as a cleidohyoid rather than the omohyoid. The muscle was innervated by a branch from ansa cervicalis and the nerve supplied the muscle from its inner aspect [Fig.2]. On the left side the cadaver exhibited a normal sternohyoid, thyrohyoid and sternothyroid muscle. Unlike the right side, typical omohyoid was present.
It is known that ontogeny recapitulates phylogeny. Such type of muscle is found in avian. Experimental embryology contributed to the understanding of the possible mechanism which may be responsible for this variation [
5]. The neural crest cells migrate and differentiate into the bones and muscle to keep the tongue skeleton (hyoid) and the pectoral girdle connected to facilitate the swallowing. The cleidohyoid stabilize the larynx during swallowing but in humans effective infrahyoid muscle group and the mylohyoid muscle have evolved to serve such purpose [
6]. Hence the human cleidohyoid muscle is thought to be the evolutionary remain from/or heritage of the avian [
6]. The incidence of anomalies of OH is high. Bergman et al. described other atypical forms of omohyoid such as: cleidofascialis, which originates from the clavicle and inserts in to the fascia colli (neck); cleidohyoideus, which originates behind the origin of the cleidomastoid part of sternocleidomastoid and inserts onto the hyoid bone; and hyofascialis, which originates from the hyoid and inserts into the omosternoclavicular fascia [
7].
There are reports of clinical cases where contracture of abnormal omohyoid muscle has caused congenital torticollis [
8,
9]. Hypertrophied omohyoid muscle can cause omohyoid syndrome leading to brachial plexus irritation [
10] and compression of the internal jugular vein [
11]. A variety of surgical interventions are performed in lower cervical region such as thyroidectomy, removal of cervical rib, transaction of scalene anterior muscle for correction of scalenus anticus syndrome and cervical lymph node dissection [
12]. In addition knowledge of such variations should be kept in mind in the diagnostic imaging studies such as interpreting MRI images of cervical region as it can be misidentified as pathologies such as lymphadenopathy, cysts, aneurysms, neurofibromas or metastases. Therefore, the radiologist and surgeons should be aware of anatomical variations in the neck [
13].
References
- Steinbach K. Uber Varietation der Unterzungenbein-und Brustmuskulatur. Anat Anz. 1923;15:488-506.
- Tubbs RS, Salter EG, Oakes WJ. Unusual origin of the omohyoid muscle. Clin Anat. 2004; 17:578-582.
- Sushma R. Kotian, Suhani Sumalatha. Cleidohyoideus Accessorius-an Additional Strap Muscle in the Neck. Cukurova Medical Journal. 2015;40 (Ek Sayi 1):102-105.
- M. Elena Stark, Bian Wu, Benjamin E. Bluth, Jonathan J. Wisco- Bilateral accessory cleidohyoid in a human cadaver. International Journal of Anatomical Variations. 2009;2:122-123.
- McGonnell IM, Mckay IJ, Graham A. A population of caudally migrating cranial neural crest cells: Functional and evolutionary implications. Developmental Biology. 2001;236:354-363.
- Chaisiwamongkol K, Sripanidkulchai K, Boonruangsri P, Toomsan Y, Teepsawang S, Songserm L. Cleidohyoid Muscle in Human: A Case Report. Srinagarind Med J. 2009; 24(3):265-267.
- Bergman RA, Thompson SA, Afifi AK, Saadeh FA. Compendium of Human Anatomic Variation. Urban & Schwarzenberg. Baltimore-Munich 1984;34:64.
- Pirsig W. Congenital torticollis with dislocation of the larynx and trachea caused by contracture of one omohyoides muscle. Arch Otorhinolaryngol. 1977;215 (3-4):335-337.
- Shih TY, Chuang JH. Fibrosis of the omohyoid muscle-an unusual cause of torticollis. J Pediatr Surg. 1998;33(5):741-742.
- Fiske LG. Brachial plexus irritation due to hypertrophied omohyoid muscle; a case report. J Am Med Assoc. 1952;149(8):758-759.
- Patra P, Gunness TK, Robert R, Rogez JM, Heloury Y, Le Hur PA, et al. Physiologic variations of the internal jugular vein surface, role of the omohyoid muscle, a preliminary echographic study. Surg Radiol Anat. 1988;10(2):107-112.
- Leppi TJ. An Anomalous Infrahyoid Muscle. The Yale Journal of Biology and Medicine. 1962;34(5):522-523.
- Bandarupalli NK, Bolla SR. Bilateral Cleidohyoideus Accessorius Muscle-A Case Report. Journal of Evolution of Medical and Dental Sciences/Volume 2/Issue 4/January 28, 2013.