Introduction
The World Health Organization (WHO) defined abortion as pregnancy termination prior to 20 weeks gestation or with a fetus born weighing less than 500 grams. It may be spontaneous or induced. Induced abortion can be further classified as therapeutic or criminal, which may be safe or unsafe [
1,
2]. Unsafe abortion is defined by the WHO as a procedure for terminating an unintended pregnancy carried out either by persons lacking the necessary skills or in an environment that does not conform to minimal medical standards, or both [
3]. Where abortion laws are restricted or safe abortion services are not widely accessible or are of poor quality like in Nigeria, women resort to unskilled providers, risking serious consequences to their health and well-being [
2,
3].
Induced abortion is illegal in Nigeria except on medical grounds to safeguard the woman’s life [
4]. However, abortions are commonly performed and due to the legal prohibition or restrictions, most abortion procedures are performed under unsafe, clandestine conditions particularly following unplanned, unintended or unwanted pregnancies [
3]. In Nigeria, according to a 2006 report, about 3000 women die annually due to unsafe abortion [
3]. The demand for abortion is most commonly seen among young unmarried women; however, it is increasingly seen even amongst married women nowadays. The problems may be related to poverty, ignorance, low level of awareness and low utilization of family planning services which may be further compounded by social and family misunderstandings or conflicts [
1-
3].
A major concern of unsafe abortion is that it is a burden on government and private health care systems as post-abortal care diminishes the system’s capacity to provide other services. To the victim, it compromises her health status and wellbeing, which could consequently affect the well-being of her family in particular and the community in general [
5-
7]. Complications resulting from induced abortion include uterine perforation, damage to the cervix and bowel perforation or prolapse. Others include hemorrhage, retained product of conception, infections, septic shock, anemia and reaction to abortificients used during procurement of the abortion. The high rate of morbidities and mortalities associated with abortions are mostly from above complications [
2,
5]. Long term complications include chronic pelvic pain, chronic pelvic inflammatory diseases, and increased risk of ectopic pregnancies, secondary infertility and psycho-social morbidities [
1,
5,
6].
We present a case of a young divorced woman who had gangrenous bowel prolapse through the vagina secondary to uterine perforation following an induced abortion. We present the surgical management of bowel injury from dilatation and curettage (D & C) and highlighted the need for basic training of medical personnel who wish to offer abortion services.
Case Report
Mrs A. Z was a 21-year-old farmer who was para 1+1. Her child was 14 months old at the time of her presentation to our center. Her husband divorced her a year prior to her presentation when the child was 2 months old. The husband was not responsible for the current pregnancy.
She was referred to our hospital with 4 days history of abdominal pain, vomiting and a day history of protrusion of intestine through her vagina. She had procured abortion of a 9-week pregnancy at a peripheral hospital about 75 kilometers from our center. The procedure described fits dilatation and curettage (D&C). She had neither analgesia nor anaesthesia. She developed moderate vaginal bleeding which was associated with colicky abdominal pain and projectile vomiting a day after the procedure. Three days later, she went back to the same hospital because of worsening symptoms. They attempted to perform another dilatation and curettage but abandoned it when they noticed protruded intestine in the vagina. She was referred to our centre the following day accompanied by her brother who shouldered the hospital bill.
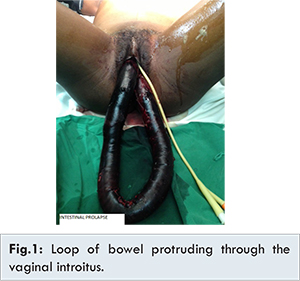
On examination, she was very anxious, moderately pale and febrile with a temperature of 38.7oC. Her pulse rate was 105 beats per minute and her blood pressure was 110/70 mmHg. The abdomen was full and markedly tender. Vaginal inspection showed a loop of bowel protruding through the vaginal introitus, approximately 80 cm long, devoid of its mesentery and gangrenous [Fig.1]. Vaginal examination showed the bowel loop protruding through the cervix. The cervix was bruised. The uterus was tender and compatible with a 10 weeks pregnancy on bimanual examination.
Her complete blood count (CBC) showed packed cell volume of 25 per cent with leucocytosis of 14x109/L; 78% of which was neutrophils. There was no remarkable derangement in the renal or liver function tests results. Pelvic ultrasound scan showed a well-defined gestational sac with mean sac diameter equivalent to 7 weeks + 1 day and a bowel shadow seen traversing the uterine cavity. She was commenced on intravenous fluids, analgesics, anti-tetanus prophylaxis and antibiotics cover comprising of ceftriaxone and metronidazole. The patient was evaluated by gynaecologists and surgeons. She consented to emergency laparotomy.
The operative findings included bulky uterus with a perforation measuring 4 cm on the posterior fundal wall [Fig.2]. Gangrenous loop of jejunum and part of proximal ileum protruded through the perforation. She had 174 cm loop of bowel resected. A single layer jejeno-ilial anastomosis, about 100 cm from the ileo-caecal junction was done. The uterine perforation was repaired in two layers after evacuation of the products of conception from below under direct vision. She had 2 pints of blood transfused.
The post-operative period was uneventful. She was discharged home after 10 days. She had post-abortion counseling with emphasis on contraception. She was followed up at the surgical clinic and gynaecology clinic for a month with no complaint. However, she was lost to follow up thereafter.
Discussion
This case highlights one of the life threatening complications resulting from illegal abortion. In Nigeria, the abortion law is restrictive with harsh penalties for both the provider of the service and the client [
4]. This provides an opportunity for quacks to offer such services often, in secrecy and in ill-equipped settings.
Our patient falls among the age groups that commonly request for abortion in Nigeria. Her decision to abort the pregnancy was based on family, social and economic reasons. She was a poor farmer, whom had been divorced and abandoned together with her child. These were the reasons given by our patient; the same reasons given by patients who seek to terminate pregnancies especially in Nigeria [
6]. This case occurred in the Northern region of Nigeria, which has been reported to have the largest proportion of complications of induced abortion caused by physicians who are mostly untrained to do this procedure [
8]. The physician involved in this case was a newly qualified doctor posted to the rural hospital who was just ‘helping’ out a pitiful young woman.
The commonest site of uterine injury is the fundus while the ileum is the most common part of bowel involved as seen in the index case [
2,
6]. In Augustin et al. [
9] reviews of D&C related bowel injury, 12 abortion-related intestinal prolapse were reported in 50 years and all of them had intestinal resection and anastomosis just as our patient did. Mabula et al. [
10] reported a sudden increase in bowel perforation from induced abortion in their centre, where dilatation and curettage was the commonest method used in 82% of their cases. Resection and anastomosis with uterine repair, as was offered to our patient, was the surgical procedure performed in 87% of their cases.
Women who had abortion complications observed that many doctors were not well trained on how to carry out abortion procedures and post abortion care [
8]. This highlights the need for training of doctors on how to do the procedure properly. The restrictive abortion law in Nigeria hinders newly qualified doctors from getting adequate training on uterine evacuation. The training during medical schools and internship were centered more on completing an incomplete abortion rather than inducing an abortion with a closed cervix requiring dilatation. When such a doctor is faced with a pressing request for termination of pregnancy like in the case presented, the consequences are but what we had seen in this case.
Conclusion
Social, family and economic reasons were mostly put forward to justify request for termination of pregnancies. However, of all of these reasons, ignorance stands out most. Ignorance and low level of awareness of contraceptive use among adolescent and young women is responsible for high rate of unwanted pregnancies resulting in termination of the pregnancy. This is further compounded by the restrictive abortion laws in most countries including Nigeria, making it difficult to have access to safe abortion services. The role of girl-child education, women empowerment, relaxation on the abortion law and proper training of personnel on abortion services cannot be over emphasized.
References
- Sudhinaraset M. Reducing unsafe abortion in Nigeria, in brief, New York; Guttmacher Institute, 2008;(30):1-4.
- Anjun R, Saher F, Gangat S, Ahmed A, Menun IA, Soomro N. Bowel injuries secondary to induced Abortion; A Dilemma. Pakist J of Surgery. 2007;23(2):122-125.
- World Health Organization (2011). Unsafe abortion: Global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008. Six editions. Geneva, WHO 2011. Available at: http://www.who.int/reproductivehealth/publications/unsafe_abortion/9789241501118/en/Accessed on March 31, 2016.
- The criminal code act (1916), chapter 77 of the laws of the federal republic of Nigeria (Reversed ed. 1990), articles 228-230. Available at: http://www.reproductiverights.org/world-abortion-laws/nigerias-abortion-provisions Accessed on March 31, 2016.
- Nkor SK, Igberase Go, Osime OC, Faleyimu BL, Babalola R. Small bowel obstruction following perforation of the uterus at induced abortion. West Afr J Med. 2009;26(5):237-339.
- Oladapo OT, Coker AA. Bowel prolapse and gangrene following vaginal Vault perforation; an example of the menace of criminal abortion in Nigeria. Trop Doct. 2005;35(3):177-178.
- Thapa SR, Rimal D, Preston J. Self-induction of abortion with instrumentation. Aust Fam Physician. 2008;35(9):697-698.
- Henshaw SK, Adewole I, Singh S, Bankole A, Oye-Adeniran B, Hussain R. Severity and Cost of Unsafe Abortion Complications Treated in Nigerian Hospitals. International Family Planning Perspective. 2008;34(1):40-50.
- Augustin G, Majerovic M, Luetic T. Uterine perforation as a complication of surgical abortion causing small bowel obstruction: a review. Archives of Gynecology and Obstetrics. 2013;288(2):311-323.
- Mabula JB, Chalya PL, McHembe MD, Kihunrwa A, Massinde A, Chandika AB, et al. Bowel perforation secondary to illegally induced abortion, a tertiary hospital experience in Tanzania. World J Emerg Surg. 2012;7(1):29.