Dilip Kumar Pal1, Pritesh Jain1, Manju Banerjee2
Departments of Urology1 and General Surgery2, Institute of Post Graduate Medical Education & Research, Kolkata-700020, West Bengal, India.
Corresponding Author:
Dr. Dilip Kumar Pal
Email: drdkpal@yahoo.co.in
Abstract
Anomalies of renal migration and fusion are rare. Ectopic kidneys that fail to ascend above the pelvic brim are commonly called pelvic kidneys. Bilateral cases have also been reported but are very rare. We present a case of 43 year old female who presented with intermittent dull aching pain in right lower abdomen, who had malrotated pelvic kidneys with vascular anomalies, associated with spina bifida. The majority of patients with ectopic kidneys are asymptomatic but those affected by obstruction, recurrent infection, or renal calculi, the anatomical position and associated anomalies should dictate the plan of management.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffacfa0f000000f204000001001500 6go6ckt5b5idvals|656 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Bilateral pelvic ectopic kidneys are rare and only few cases are reported in the medical literature [1]. Most common type of renal ectopia is the pelvic kidney whose incidence is estimated from 1 of 2100 to 3000 autopsies [2]. Infection and calculus can affect ectopic kidneys, leading to non-classical abdominal pain. The abnormalities in the renal arteries are mainly due to the various developmental positions of the kidney [3]. In our case, bilateral pelvic kidneys with anomalous origin of renal arteries associated with spina bifida were present. To our knowledge bilateral pelvic kidneys have also been reported but are very rare.
Case Report
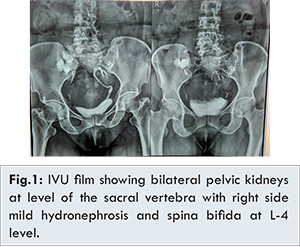
A 43 year old female presented with complaints of intermittent dull aching pain in right lower abdomen since the past 3 years. She also had lower back pain radiating to right lower limb from last few days. General physical examination revealed no abnormalities. She was normotensive. On laboratory investigations she was normoglycemic with normal renal biochemical parameters. Urine analysis was normal. On screening ultrasound bilateral ectopic kidneys were found with hydronephrotic changes in right kidney. Intravenous urogram (IVU) showed bilateral pelvic kidneys at the level of sacrum with associated malrotation and mild hydronephrosis on right side with good excretion of contrast through both kidneys. Spinal abnormalities were also noted at L-4 vertebral level [Fig.1].
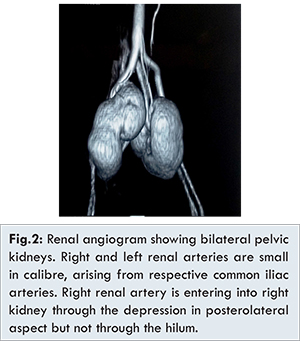
Contrast enhanced computed tomography (CECT) of kidney-ureter-bladder (KUB) region with renal angiography showed bilateral ectopic kidneys in pelvis. Left kidney was normal in size (9.4 cm), shape, outline and enhancement. Left renal artery originated from left common iliac artery near bifurcation of aorta entering into the hilum of the kidney and was very small in calibre. Right kidney was normal in size (10.6 cm), shape, outline and enhancement, however a prominent extrarenal pelvis was present. Right renal artery was also very small in calibre and originated from right common iliac artery. Right renal artery was entering into the kidney through a depression in the posterolateral aspect but not through the hilum. Right and left renal vein were coming out of the hilum and was entering into the proximal inferior vena cava [Fig.2]. DTPA renogram did not show any obstruction to right kidney. She was managed conservatively and was referred to neurologist regarding vertebral anomalies and associated lower back pain.
During embryologic development kidneys ascent to their normal retroperitoneal position, any arrest or abnormal migration leads to ectopic location of that kidney. Several pathologies may be related to congenital anomalies of urinary tract, 40% of these pathological conditions are due to variations in number, position, shape, and size of the kidney, ureter, or bladder [4]. Between the sixth and ninth weeks of intrauterine life, the kidneys ascend to the lumber region just below the adrenal glands, along the dorsal aorta. The precise mechanism for this ascent is not known, but it is speculated that an inductive substance secreted by the kidneys and differential growth of the lumbar and sacral regions of the embryo plays a major role [2]. The factors that may interfere with the renal developmental anomalies are teratogenic agents, genetic factors, chromosomal abnormalities, disorders in fusion mechanism of the ureteric bud with metanephric blastema, and various medications ingested by the mother [5]. Ectopic kidneys may be associated with other congenital anomalies with genital anomalies being the most common (15%-45%) [6]. In our case bilateral pelvic kidneys were present just lateral to midline at the sacral level. This position suggests that factors have affected the renal ascent as well as the rotation process but the growth of the kidney was not affected. There is a good correlation between kidney ascension and the level of origin of the renal arteries, any anomaly in the renal artery development may delay kidney migration [7]. In the present case both of the kidneys have undergone incomplete rotation. Kidneys in pelvic position may go undetected in life and get noticed either in autopsy or during dissection. Anatomical variations regarding the vascularization of kidneys like multiple arteries are also associated with congenitally abnormal kidneys. Renal arteries anomalies are much more common than anomalous renal veins [8]. The pelvic kidney may be affected by the same disease process that affect the normal positioned kidneys but due to its non-anatomical position, vascular anomalies and associated anomalies when affected by some disease it provides a unique challenge to the surgeons. Pelvic kidney with rotational variation though comparatively rare assumes great importance in view of present day surgical procedures like laparoscopic and robotic radical nephrectomy, percutaneous nephrolithotomy, and renal transplantation. A pelvic kidney presents challenges to clinician including limited working space, proximity of vital structures including the great blood vessels, anomalous hilar structures, and difficulty encountered in optimal port placements. Because of the greater risk of injuring aberrant vessels or overlying abdominal viscera and nerves, the pelvic kidney presents special treatment challenges. Multi-slice CT and 3D-CT angiography is an appropriate imaging modality when surgery is required for removal of an ectopic kidney [9]. Pregnancy and labour with maternal renal pelvic ectopia provides a unique challenge to the obstetricians attempting to prevent damage to the kidneys during labour and allow safe delivery [10]. Usually if accessory renal arteries are present they have longer length and small diameter, in our case both main renal arteries were longer in length and of very small calibre so whole of the kidney supported by these main renal arteries may display lower blood pressure which may cause hypertension by stimulating renin secretion. In addition to this, these narrow calibre arteries will be easily affected by any atherosclerotic process, so regular follow up and strict vigilance is required to prevent or control of various factors which may predisposed to metabolic syndrome.
Conclusion
Bilateral pelvic kidneys associated with vascular anomalies and malrotation is a very uncommon anomaly. The scenario will be more complicated if pelvic kidney is associated with anomalies of other organ systems. The knowledge of the possibility of this anatomical variation will be of help to the clinician in making correct diagnosis and offering appropriate treatment.
References
- Arch E. Bilateral pelvic kidney. J Urol. 1966;49:977-978.
- Bauer SB. Anomalies of the upper urinary tract. In: Wein A, Campbell-Walsh Urology. 11th ed. Saunders Elsevier: Philadelphia; 2016. pp. 2985-86.
- Moore KL, Persaud TVN. The Developing Human: Clinically Oriented Embryology. 10th edition. WB Saunders: Philadelphia, PA, USA;2015. pp. 242-45.
- Williams PL, Bannister LH, Berry MM. Gray’s anatomy in embryology & development, Urinary System, Churchill Livingstone, London, UK, 38th edition. 1995; pp. 199-204.
- Gulsun M, Balkanci F, Ekirge SC, Deger A. Pelvic kidney with an unusual blood supply angiographic findings. Surgical and Radiologic Anatomy. 2000;22:59-61.
- Downs RA, Lane JW, Burns E. Solitary pelvic kidney, its clinical implications. Urology. 1973;1:51-56.
- Govindarajan A, Meenakshisundaram J. Right ectopic kidney with rare vascular variations Right ectopic kidney with rare vascular variations. International Journal of Anatomical Variations. 2011;4:12-14.
- Gillaspie C, Miller LI, Baskin M. Anomalous renal vessels and their surgical significance. Anat Rec. 1916;11:77.
- Mahmoudnejad N, Danesh A, Abdi H. Renal cell carcinoma in presacral pelvic kidney. J Pak Med Assoc. 2009;59:482-483.
- Meizner, Barnhard Y. Bilateral fetal pelvic kidneys: documentation of two cases of a rare prenatal finding, Journal of Ultrasound in Medicine. 1995;14:487-489.
|