6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa4d0160000003b05000001000100
6go6ckt5b5idvals|731
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
CA-125 (cancer antigen 125 or carbohydrate antigen 125) is a protein secreted normally by human body in small quantities [
1]. It is usually associated with benign conditions if mildly raised, and very high levels indicate malignancy (normal value <35 U/mL) [
2]. Most frequently it is used as a biomarker for epithelial ovarian cancer. However, it has limited specificity, i.e. it can be raised in other conditions also, like, diverticulitis, liver cirrhosis, normal menstruation, pelvic inflammatory disease, pregnancy or uterine fibroids [
3,
4]. CA-125 levels more than 65 U/mL in a postmenopausal female with a palpable adnexal mass are predictive of ovarian malignancy in >95% cases [
5]. There is a need for careful clinical evaluation in cases which present with high levels of CA-125 as some cases have been reported in literature, which, on histopathological examination, were found to be endometriomas [
6-
10].
Case Report
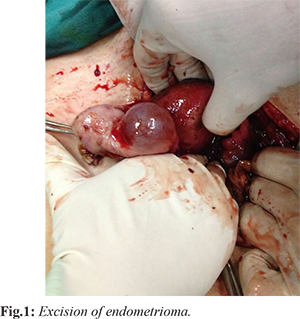
Two ladies presented with pain abdomen in gynaecology outpatient department. On careful evaluation, adnexal masses were discovered associated with very high CA-125 levels. Our first case was a 40 year old unmarried female (nulliparous) who presented with pain in lower abdomen. On per abdomen examination abdomen was soft, no mass was felt. On per rectal examination, a left adnexal mass of approximately 6 x 5 cm was found, which on ultrasonography, showed a cystic structure originating from left ovary of size 6.5 x 4.7 cm with mild ascites. CECT confirmed the findings. CA-125 levels were 908 U/mL. Exploratory laparotomy was planned for the patient and a large left ovarian cyst was removed (left salpingoophorectomy was done) [Fig.1]. The histopathological examination confirmed endometrioma. CA-125 levels reduced to 21.40 U/mL within 3 weeks after the surgery. No recurrence was reported on follow up of the patient.
In the second case, a 43 year old P2L2 lady presented with chief complaints of pain lower abdomen. Her per vaginal examination was suggestive of bilateral adnexal masses and ultrasound showed bilateral large ovarian cysts of approximately 6 x 7 cm. A metastatic work-up revealed CA-125 levels of 4420.90 U/mL (high), CA-19.9 levels of 3224.84 U/mL (high), CEA levels of 1.72 ng/mL (normal). A laparotomy was planned in which total abdominal hysterectomy with bilateral salpingoophorectomy with omental biopsy was done. Peroperatively, both ovaries were enlarged. On the right side, cyst was ruptured with contents spilled onto the peritoneum. Left cyst was intact. Gut was adhered to bilateral ovarian masses. CA-125 levels dropped to 1450 U/mL within one week after surgery, reaching 37 U/mL after 6 weeks on follow up. Histopathology revealed endometriotic cysts with no neoplastic changes. Omental biopsy was within normal limits.
Discussion
In 1981, CA-125 was identified as an ovarian cancer antigen and was investigated as a specific marker of ovarian malignancy. The reference value of 35 IU/mL was based on the pioneering work by Bast et al. [
11]. A serum CA 125 level of more than 200 U/mL is considered a positive criterion for differentiating malignant from benign pelvic masses in premenopausal women younger than 50 years [
12]. It is generally believed that the higher the serum CA 125 value, the greater is the probability that the abdomino-perineal mass is malignant. In normal women, plasma concentrations of CA125 are increased slightly at ovulation and significantly during menstruation. Marked increases are observed during pregnancy and following peritoneal irritation by infection or surgery [
13]. High levels of CA-125 usually lead to a presumptive diagnosis of ovarian cancer.
Plasma concentrations of CA-125 are markedly elevated in women with cystic ovarian endometriosis and/or deeply infiltrating endometriosis, but not, or only slightly, in the luteal phase of women with minimal or mild endometriosis. This is consistent with the recent concept which considers minimal endometriosis as a normal condition occurring intermittently in many women, in contrast with deep endometriosis and cystic ovarian endometriosis which are called ‘endometriotic disease’. Serum CA125 is not a good marker for endometriosis but it is a helpful additional parameter to diagnose endometriotic disease in patients with chronic pelvic pain [
13]. Following treatment of endometriosis, elevated plasma concentrations of CA125 could be used as an argument that treatment has been incomplete, or that the condition has recurred. There is evidence that peritoneal mesothelial cells are even more potent than ovarian cancer cells in producing CA-125 [
14]. The overflow of thick, ‘chocolate’ cyst fluid in the peritoneal cavity causes endometriosis-induced peritoneal inflammation [
15] which leads to excess CA-125 in the circulation. In addition, superficial endometrial implants over the ovary may secrete CA-125 into the peritoneal cavity which further gets reabsorbed slowly into the circulation.
The persistently high serum CA-125 level for more than 2 months supports the concept that mesothelial cells of the peritoneum were the most important source of CA-125 in the present case. However, a benign pathology like endometrioma should also be considered. In the literature review, very few cases are reported wherein high levels of CA-125 are found in endometriotic cysts. Accurate diagnosis, high clinical suspicion and histopathologic report are essential to prevent unnecessary surgical exploration and correct diagnosis.
Conclusion
The possibility of endometrioma should definitely be considered as a clinical diagnosis in cases of adnexal mass with high levels of CA-125, even in the absence of widespread endometriosis.
Contributors: DT: Report conception and initial manuscript drafting; SG: Critical review of manuscript; AB: Manuscript revision. All authors were involved in case management. SG will act as guarantor. All authors approved the final version of the manuscript.
Funding: None; Competing interests: None stated.
References
- Bast RC, Xu FJ, Yu YH, Barnhill S, Zhang Z, Mills GB. CA 125: the past and the future. The International Journal of Biological Markers.1998;13:179-187.
- Alagoz T, Buller RE, Berman M, Anderson B, Manetta A, DiSaia P. What is a normal CA125 level? Gynecol Oncol. 1994;53:93-97.
- Faulkner D, Meldrum C. Tumour markers. Australian Prescriber. 2012;35:125-128.
- Sarandakou A, Protonotariou E, Rizos D. Tumor markers in biological fluids associated with pregnancy. Critical Reviews in Clinical Laboratory Sciences. 2007;44:151-178.
- Fritsche HA, Bast RC. CA 125 in ovarian cancer: advances and controversy. Clinical Chemistry. 1998;44:1379-1380.
- Asher V, Hammond R, Duncan TJ. Pelvic mass associated with raised CA 125 for benign condition: a case report. World Journal of Surgical Oncology. 2010;8:28.
- Ghaemmaghami F, Karimi ZM, Hamedi B. High levels of CA125 (over 1,000 IU/ml) in patients with gynecologic disease and no malignant conditions: three cases and literature review. Arch Gynecol Obstet. 2007;276:559-561.
- Kahraman K, Ozguven I, Gungor M, Atabekoglu CS. Extremely elevated serum CA-125 level as a result of unruptured unilateral endometrioma: the highest value reported. Fertil Steril. 2007;88(4):968.
- Muyldermans M, FJ Cornillie FJ, Koninckx PR. CA125 and endometriosis. Hum Reprod Update. 1995;1(2):173-187.
- Phupong V, Chen O, Ultchaswadi P. High level of CA 125 due to large endometrioma. J Med Assoc Thai. 2004;87:1108-1111.
- Bast RC, Jr, Klug TL, St John E, Jenison E, Niloff JM, Lazarus H, et al. A radio-immunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N Engl J Med. 1983;309:883-887.
- Graham L. ACOG releases guidelines on management of adnexal masses. Am Fam Physician. 2008;77(9):1320-1323.
- Muyldermans M, Cornillie FJ, Koninckx PR. CA125 and endometriosis. Hum Reprod Update. 1995;1:173-187.
- Zeimet AG., Marth C, Offner FA, Obrist P, Uhl-Steidl M, Geichtinger H. Human peritoneal mesothelial cells are more potent than ovarian cancer cells in producing tumor marker CA-125. Gynecol Oncol. 1996;62:384-389.
- Bouquet de Joliniere J, Validire P, Canis M, Doussau M, Levardon M, Goqusev J. Human endometriosis-derived permanent cell line (FbEM-1): establishment and characterization. Hum. Reprod Update. 1997;3:117-123.