|
Maria Kouroupi1, Efthimios Sivridis1, Stella Arelaki1, Paschalis Askitis2, Alexandra Giatromanolaki1 1Department of Pathology, Democritus University of Thrace, Alexandroupoli, Greece; 2Department of Ear, Nose and Throat, University General Hospital of Alexandroupoli, Alexandroupoli, Greece.
Corresponding Author:
Dr. Maria Kouroupi Email: marykouroupi@gmail.com
Abstract
Background: Plasmacytomas are characterized by excessive proliferation of neoplastic plasma cells in the bone marrow. Extra-medullary plasmacytoma are by and large, encountered in the head and neck region and only rarely occur in the tonsils. Case Report: We report here a asymptomatic solitary non-secreting plasmacytoma of the right tonsil in a middle-aged woman. The diagnosis of a plasmacytoma was reached after surgical excision. Conclusion: Tonsil is a rare sight of plasmacytoma origin with no specific symptoms, thus recommendation of WHO 2015 for such tumors must be taken under consideration.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffe4b3200000002507000001000700 6go6ckt5b5idvals|841 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Solitary extra-medullary plasmacytoma is defined as a localized tumor consisting of monoclonal plasma cells, with no other bone lesions or organ involvement and without any clinical manifesta-tions of myeloma (WHO 2015) [ 1]. Extra-medullary plasmacytomas usually occur in the head and neck region (80%) [ 2, 3], with the nasopharynx and sinonasal cavities being the most common sites [ 4- 6]. Involvement of the tonsil is unusual [ 7, 8] with only a few cases having been reported. Incidence is more in men (75%) [ 9].
Case Report
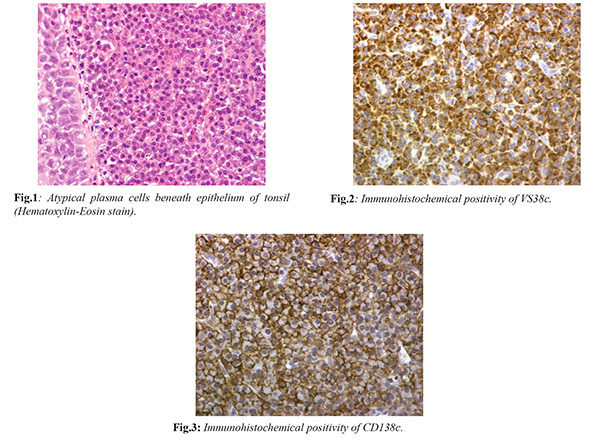
A 62-year-old woman attended the ear, nose and throat clinic with complaints of lump sensation during the last three months, recently becoming mild odynophagia. Physical examination revealed a slight enlargement of the right tonsil. She had no relevant past history or any overt systemic symptoms. Laboratory findings were normal: white blood cells were 6.33 K/µl, hematocrit 41.3% and hemoglobin 14.2 g/dL. The patient’s coagulation mechanism was within normal limits (prothrombin time 10.4 seconds, INR 0.89, APTT 26.70 seconds and platelet count was 306 K/µL). Blood examination showed normal concentration of glucose (105 mg/dL), serum urea (39 mg/dL), creatinine (0.7 mg/dL), potassium (4.6 mmol/L) and sodium (144 mmol/L). Blood immunoglobulin assays IgA, IgG, IgM were unremarkable with values reaching 333 mg/dL, 1020 mg/dL and 241 mg/dL, respectively, while light chains ? and ? were normal (15 mg/L each). Magnetic resonance imaging was within normal limits. With these normal laboratory findings, a provisional diagnosis of an inflammatory process was made, and antibiotic treatment was given. There was no response and the patient was subjected to excisional surgery. Microscopically, there was a diffuse monomorphic infiltrate composed of medium sized, atypical plasma cells, with large rounded eccentric nuclei, prominent nucleoli, and abundant finely granular cytoplasm [Fig.1]. The cells were immune-histochemically positive for CD 79a (Biocare, mouse monoclonal, HM47/A9), VS38c [Fig.2] (Dako, plasma cell mouse monoclonal clone VS38c), CD138 [Fig.3] (Dako, mouse monoclonal, M15), IgA (Dako, rabbit polyclonal), ? light chain (Dako, rabbit polyclonal), and they were negative for ? light chain (Dako, rabbit polyclonal), and the markers CD3 (Dako, mouse monoclonal, F72.38), CD20 (Dako, mouse monoclonal, L26), IgG (Dako, rabbit polyclonal), IgM (Dako, rabbit polyclonal), IgD (Dako, rabbit polyclonal) and IgE (Dako, rabbit polyclonal). With the preliminary diagnosis of a plasma cell neoplasm the patient underwent bone marrow biopsy for further assessment: this showed reactive changes only. On the basis of these investigations, a solitary extra-medullary non-secreting plasmacytoma was established. The patient is presently under continuous follow up, with no recurrence for the last four years.
Discussion
Plasmacytomas occurring in the tonsils are extremely rare, but this case is unique for it is non-secretory. Another non-secretory case was reported in a man by Sakai Y et al. [ 7]. A study by Alexiou et al. [ 10] described 75 cases of extra-medullary plasmacytoma many of which were on the palate region. However, they failed to mention whether any case was non-secretory in nature. With the exception of one case reported in the literature, all presented with mild symptoms. The exception was a single case of a man with plasmacytoma located on the left tonsil with prominent tonsillar enlargement which produced airway obstruction and sleep apnea [ 11]. For no apparent reasons, plasmacytomas occur mainly in men (3:1) and on the left side. Bazzadut et al. and Ramachandra et al. reported a case of a male patient concerning the right one [ 12, 13]. Furthermore, a single case of bilateral tonsillar plasmacytoma has been reported [ 14, 15], as well as a case of a plasmacytoma of tonsil with synchronous oral squamous cell carcinoma [16].
The diagnosis of a plasmacytoma is usually straightforward and is based on the presence of atypical plasma cells and monoclonality. It is essential that the presence of disseminated disease is excluded after a meticulous laboratory and imaging tests. Laboratory studies include biochemical blood examination, in addition to serum protein electrophoresis and immunofixation, ß2-macroglobulin assay, urine Bence-Jones proteins and bone marrow examination. Imaging examination involves radiologic skeletal survey, magnetic resonance imaging of spine, pelvis, humerus and femurs. Treatment of such neoplasm includes radiotherapy following surgery [ 8, 15]. 25% of all solitary cases will recur and 10-20% will eventually develop multiple myeloma [ 3], up to 12 years after the initial diagnosis. Predictive value for the development of multiple myeloma seems to have the presence of nuclear immaturity with prominent nucleoli. Local recurrence of the lesion is uncommon.
Conclusion
This rare case of tonsillar plasmacytoma presented with mild, non-specific symptoms, suggesting an inflammatory process with the unique feature of IgA production without secretion. The WHO 2015 recommendation for such rare cases should always be taken into consideration.
Contributors: MK: drafting of manuscript; ES: manuscript writing and revision for intellectual content; SA, PA: critical inputs in manuscript and collection of clinical data; AG: critical revision and study supervision. MK will act as guarantor. All authors approved the final version of this manuscript. Funding: None; Competing interests: None stated.
References - WHO classification of tumours of haematopoietic and lymphoid tissue 4th edition. 2015.
- Poole AG, Marchetta FC. Extramedullary plasmatocytoma of the head and neck. Cancer. 1968;22:14-21.
- Kapadia SB, Desai U, Cheng VS. Extramedullary plasmacytoma of the head and neck. A clinicopathologic study of 20 cases. Medicine (Baltimore). 1982;61:317-328.
- Bachar G, Goldstein D, Brown D, Tsanq R, Lockwood G, Perez-Ordonez B, et al. Solitary extramedullary plasmacytoma of the head and neck-Long-term outcome analysis of 68 cases. Head and Neck. 2008;30:1012-1019.
- Miller FR, Lavertu P, Wanamaker JR, Bonafede J, Wood BG. Plasmacytomas of the head and neck. Otolaryngology-Head and Neck Surgery. 1998;119:614-618.
- Kalan A, Asare-Owusu L, Tariq M. Solitary extramedullary plasmacytoma of tonsil - a rare location. Indian J Otolaryngol Head Neck Surg. 2000;52:285-289.
- Sakai Y, Ikeya J, Morita I, Sato K. Extramedullary plasmacytoma of the tonsil diagnosed by fine-needle aspiration cytology. Annals of Diagnostic Pathology. 2008;12:41-43.
- Tokatli F, Puyan FO, Alas RC, Tuncbilek N, Uzal C. Extramedullary plasmacytoma: clinicopathology, immunohistochemistry and therapeutic approach to a case with a tonsillar site. Hematology/Oncology and Stem Cell Therapy. 2008;1:241-245.
- Röcken C, Hegenbarth V, Schmitz M, Stix B, Schade G, Mohnert A, et al. Plasmacytoma of the tonsil with AL amyloidosis: evidence of post-fibrillogenic proteolysis of the fibril protein. Virchows Arch. 2000;436:336-344.
- Alexiou C, Kau RJ, Dietzfelbinger H, Kremer M, Spiess JC, Schratzenstaller B, et al. Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts. Cancer. 1999;85:2305-2314.
- Huoh KC, Van Zante A, Eisele DW. Extramedullary plasmacytoma of the tonsil. Case Rep Otolaryngol. 2011;2011:430809.
- Bhat RV, Prathima KM, Kumar H, Narayana GK. Plasmacytoma of tonsil diagnosed by fine-needle aspiration cytology. J Cytol. 2010; 27:102-103.
- Hanna EY, Lavertu P, Tucker HM, Tubbs RP. Bilateral extramedullary plasmacytomas of the palatine tonsils: a case report. Otolaryngol Head Neck Surg. 1990;103:1024-1027.
- Soutar R, Lucraft H, Jackson G, Reece A, Bird J, Low E, et al. Working Group of the UK Myeloma Forum; British Committee for Standards in Haematology; British Society for Haematology. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Clin Oncol (R Coll Radiol). 2004;16:405-413.
- Junquera L, Gallego L, Torre A, Hernando J, Fresno MF. Synchronous oral squamous cell carcinoma and extramedullary plasmatocytoma of the tonsil. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:413-416.
|