6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff64e6220000007007000001000200
6go6ckt5b5idvals|866
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Acute appendicitis is one of the most common general surgical conditions encountered. However, blunt abdominal trauma as a cause of appendicitis has been only rarely reported since the 1930s [
1]. One of the first accounts is related to the famous magician Houdini, who allowed himself to be punched in the right side of his abdomen as a show of strength. He then passed away with cause of death being listed as peritonitis secondary to perforated appendicitis. This was one of the first documentations linking trauma as a possible cause of appendicitis. Despite this, controversy has remained whether the diagnosis of appendicitis in a traumatic setting is a causal or coincidental finding. Given the morbidity and mortality associated with undiagnosed appendicitis, there should be a high degree of suspicion in a patient presenting with abdominal pain following recent trauma. Here, we present a case report of a 22 year old male with traumatic appendicitis.
Case Report
A 22 year old previously fit and well male was admitted to the emergency department after falling from a ladder (approximately 3 meters) and landing on a concrete floor. He landed on his right side and initially complained of pain in his right shoulder and lateral right hip. He was brought directly to hospital by his colleague.
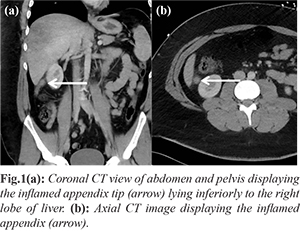
On examination, his vital signs were satisfactory (heart rate: 89 beats per minute, blood pressure: 126/85 mmHg, oxygen saturation 98% on room air, respiratory rate 12 per minute) and he was afebrile. His primary survey revealed tenderness in the right upper quadrant of his abdomen but no other significant findings. Secondary survey revealed soft tissue swelling over the right antero-lateral shoulder and lateral right hip. Musculoskeletal X-rays revealed no bony injuries. Subsequent outpatient MRI right shoulder revealed a full thickness supraspinatus tear. Blood investigations including inflammatory markers were normal (total leukocyte count: 7.5×109/L, C-reactive protein: 1.7 mg/L). A CT abdomen/pelvis was performed 3 hours post-fall as his right sided abdominal pain became more severe. The CT scan displayed an inflamed and distended distal appendix, the tip of which was located in the right upper quadrant. The radiological diagnosis was of acute appendicitis [Fig.1a,b] with no other significant abnormalities noted. On closer questioning he had been fit and well prior to his fall and denied any other constitutional symptoms.
He proceeded to have a diagnostic laparoscopy where an inflamed retro-caecal appendix consistent with acute appendicitis was identified. The tip of the inflamed appendix was located within the right upper quadrant immediately underlying the inferior border of the right liver lobe [Fig.2a]. There was no injury to surrounding organs noted. Appendicectomy was performed and the excised specimen was sent to pathology [Fig.2b]. The patient underwent an uneventful post-operative recovery.
The final histopathology examination demonstrated active inflammatory changes consistent with acute appendicitis [Fig.3a]. A vessel within the inflamed peri-appendiceal adipose tissue showed an acute inflammatory infiltrate [Fig.3b]. Subsequent outpatient colonoscopy only revealed diverticulosis of the sigmoid colon with no other abnormalities.
Discussion
Appendicitis following trauma is a rare sequalae. It has been previously reported following blunt abdominal trauma including falls, road traffic accidents, assault, bicycle handle and crush injures [
2,
3]. The patho-physiology of non-traumatic acute appendicitis has been thought to be due to obstruction of the proximal appendiceal lumen leading to a cycle of distension, impaired blood flow and bacterial multiplication, eventually leading to perforation. However, this remains unproven and has also been challenged [
4]. In cases of traumatic acute appendicitis, a number of theories have been proposed. Paschos et al. [
5] proposed that external traumatic pressure can lead to edema or hematoma of the caecum and appendix with resultant hyperplasia of intrinsic lymphoid tissue, that in turn can lead to increased caecal pressure and distension of the appendix. This in turn leads to reduced visceral arterial pressure resulting in appendicitis. Ramsook et al. [
6] propose that trauma leads to increased intra-abdominal pressure leading to increased intra-caecal pressure resulting in appendiceal distension causing appendicitis. Direct appendiceal trauma in the presence of an appendiceal faecolith has also been thought to cause an increase in intra-luminal pressure leading to mucosal fissures allowing bacterial invasion into the submucosa [
3]. According to Wani [
7], the most common reason for traumatic appendicitis is a retrocaecal appendix, because in other positions the appendix is protected by intervening small bowel.
A few studies [
6,
8-
10], old and more recent, have proposed specific diagnostic criteria for traumatic appendicitis. A combined summary of these include: (i) no history of previous attacks of appendicitis or abdominal complaints prior to trauma; (ii) direct trauma to abdominal wall or acute, unexpected, severe indirect trauma; (iii) symptom onset soon after trauma; (iv) symptoms should persist and progress with surgical confirmation of appendicitis.
The signs and symptoms of appendicitis may not be initially obvious following trauma. The clinician should have a high degree of suspicion in someone presenting with abdominal pain following a traumatic incident, as it is bound to carry medico-legal implications if missed. This should include a complete history with serial physical examinations if necessary, as well as inclusion of imaging studies including CT abdomen/pelvis.
Conclusion
Despite the poorly understood patho-physiological mechanism, traumatic appendicitis appears to be rare sequelae of blunt abdominal injury. In this era, no one should have to die from a missed diagnosis of appendicitis. Physicians and surgeons need to be mindful and highly suspicious of this rare condition when assessing patients after blunt abdominal traumas who display signs of right sided abdominal tenderness.
Contributors: JS: manuscript writing, patient management; RO, ZYY: manuscript editing, patient management;
MS: critical inputs into the manuscript and patient management. JS will act as guarantor. All authors approved the final version of this manuscript.
Funding: None; Competing interests: None stated.
References
- Hennington MH, Tinsley EA, Proctor HJ, Baker CC. Acute appendicitis following blunt abdominal trauma. Incidence or coincidence? Annals of Surgery. 1991;214:61-63.
- Bouassria A, Ibn Majdoub K, Yazough I, Ousadden A, Mazaz K, Taleb KA. Traumatic appendicitis: a case report and literature review. World Journal of Emergency Surgery. 2013;8:31.
- Toumi Z, Chan A, Hadfield MB, Hulton NR. Systematic review of blunt abdominal trauma as a cause of acute appendicitis. Annals of The Royal College of Surgeons of England. 2010;92:477-482.
- Petroianu A, Villar Barroso TV. Pathophysiology of acute appendictis. JSM Gastroenterol Hepatol. 2016;4(3):1062.
- Paschos KA, Boulas K, Liapis A, Georgiou E, Vrakas X. Traumatic appendicitis in minor blunt abdominal injury. Emergency Medicine Australasia. 2012;24:343-346.
- Ramsook C. Traumatic appendicitis: fact or fiction? Pediatric Emergency Care. 2001;17:264-266.
- Wani I. Post-traumatic retrocaecal appendicitis. OA Case Reports. 2013; 2(4):31.
- Fowler RH. The rare incidence of acute appendicitis resulting from external trauma. Ann Surg. 1938;107:529-539.
- Cobb T. Appendicitic following blunt abdominal trauma. Am J Emerg Med. 2017; 35:1386.e5-1386.e6
- Rhodes GK, Birnbaum WD. Traumatic appendicitis. Cal West Med. 1940;53:162-165.