6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff24bb24000000f106000001000800
6go6ckt5b5idvals|888
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Amyloidosis is defined by extracellular deposition of amyloid fibrils in a variety of organs and tissues. Deposits can be either localized or with systemic involvement. These deposits interfere with the normal anatomical structure of the organ and eventually leading to impairment of their function [1]. Localized deposits are usually benign in nature, but not in its systemic form.
Primary laryngeal amyloidosis is a rare lesion accounting for 0.2-1.2% of benign tumors of larynx [1,2]. Larynx is the most common site of amyloid deposition in head and neck region. [3]. Hence we report a case of primary laryngeal amyloidosis.
Case Report
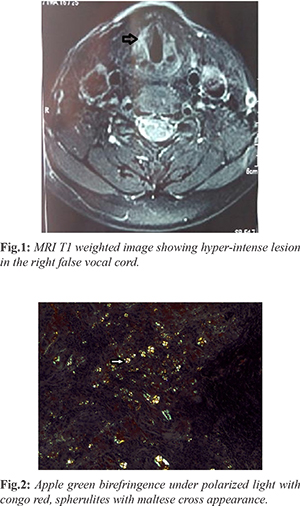
A 60 year old post-menopausal lady presented with complaints of hoarseness of voice for one month duration. She had no other complaints, known co-morbid illnesses or family history of cancer. Her Eastern Cooperative Oncology Group (ECOG) performance status was 1. General physical examination and systemic examinations were normal. On evaluation with direct laryngoscopy she had an abnormal irregular bulge in the right vocal cord. MRI neck done showed an ill defined mass lesion measuring 15.2×6.2 mm in the false cord extending anteriorly into the midline, superior extension into the supraglottic space with mild extension into the paraglottic fat noted [Fig.1]. Oesophago-gastro-duodenoscopy showed a submucosal bulge in right supraglottic area with both vocal cord mobile. Biopsy was taken from the lesion which was reported as multiple tissue fragments with focal surface respiratory type epithelial lining at places, stroma contained multiple foci of homogenous appearing eosinophilic material with irregular margins and well formed globules morphology favoring amyloidoma. Congo red stain highlighted amyloid deposit which under polarized light showed characteristic apple green birefringence. Amyloid spherulites were also noted with characteristic maltese cross appearance under polarized light [Fig.2].
The next step was to rule out systemic amyloidosis, serum free light chain and ultrasound abdomen was done, both the investigations were normal. Thus a diagnosis of localized amyloidoma larynx was done and she underwent endoscopic resection of the mass and now she is on regular follow up.
Discussion
In amyloidosis there is extracellular protein fibril deposition in various tissues. Amyloidosis is broadly classified into systemic and localized amyloidosis. Systemic amyloidosis is further sub-classified into (i) hereditary with amyloid transthyretin protein amyloid (ATTP), (ii) idiopathic with light chain amyloid (AL), (iii) secondary or reactive amyloidosis due to chronic infection or proliferation of underlying tumor proliferation with acquired amyloid (AA) [4].
In respiratory tract true and false vocal cord are the most common sites of localized amyloidosis. Other sites include ventricles, eyes, orbits, salivary glands, para-nasal sinuses, oral cavity, nasopharynx, nose and lungs [5]. Oral and para-nasal amyloidosis are more often systemic amyloidosis with an underlying plasma cell dyscrasia. They most commonly present in the age group of 50-70 years. Laryngeal amyloidosis most commonly presents with hoarseness, other associated symptoms could be dyspnoea, dysphagia [2,6]. In our case age of patient was 60 years and she also presented with hoarseness of voice.
For evaluation the choice of imaging modality is MRI where the lesion appears iso-intense in T1 weighted sequence and remains iso or slightly hyper intense in T2 weighted image. In our patient MRI showed irregular ill defined lesion in false vocal cord extending anteriorly into mid line, superiorly into supraglottic space with mild extension into paraglottic fat. Diagnosis is usually clinched using histological appearance and positive stain to Congo red, which shows a classical appearance of apple green birefringence under polarized light [7]. In this study histologically we noted a multiple foci of homogenous eosinophilic material with irregular margins and also well formed globules favoring amyloidoma. Congo red stain highlighted amyloid deposits which under polarized light show characteristic apple green birefringence. Amyloid spherulites are also noted with characteristic maltese cross appearance under polarized light which is a rare presentation.
Once the diagnosis of laryngeal amyloidosis is made, further evaluations should be made to rule out systemic disease. Serum free light chain electrophoresis, ultrasound abdomen, electrocardiogram, echocardiography, tuberculin skin test, antinuclear antibody, rheumatoid factor should be carried out [2]. We also ruled out systemic involvement.
Treatment of primary localized amyloidoma larynx is surgical resection which can be done with the aid of laser technology and endoscopic CO2 laser excision as the first line of therapy [8]. A regular follow up with laryngoscopy is suggested. Our patient also underwent endoscopic surgical resection and currently on follow up.
Conclusion
Laryngeal amyloidoma is an uncommon disorder of localized amyloidosis. Being a rare disorder, systemic pre-disposition should be evaluated and excluded meticulously. The diagnosis of amyloidosis should be confirmed histologically. Surgical resection is the mainstay of treatment.
Contributors: AR: data acquisition and manuscript preparation; NM: concept and manuscript review; BR: definition of intellectual contents, design and manuscript editing; BM: literature search and review. NM will act guarantor of the study. All authors approved the final version of this manuscript.
Funding: None; Competing interests: None stated.
References
- Thompson LDR, Derringer GA, Wenig BM. Amyloidosis of the larynx: A clinicopathologic study of 11 Cases. Modern Pathology. 2000;13:528-535.
- Behnoud F, Baghbanian N. Isolated laryngeal amyloidosis. Iran J Otorhinolaryngol. 2013;25:49-52.
- Raymond AK, Sneige N, Batsakis JG. Amyloidosis in the upper aerodigestive tracts. Annals of Otology, Rhinology & Laryngology. 1992;101:794-796.
- Yiotakis I, Georgolios A, Charalabopoulos A, Hatzipantelis P, Golias C, Charalabopoulos K, et al. Primary localized laryngeal amyloidosis presenting with hoarseness and dysphagia: a case report. Journal of Medical Case Reports. 2009;3(1):9049.
- Pietruszewska W, Wagrowska-Danilewicz M, Klatka J. Amyloidosis of the head and neck: a clinicopathological study of cases with long term follow-up. Archives of Medical Science. 2014;4:846-852.
- Daudia A. Primary amyloidosis of the larynx. Postgraduate Medical Journal. 2000;76(896):364-365.
- Utz JP. Pulmonary Amyloidosis. The Mayo Clinic Experience from 1980 to 1993. Annals of Internal Medicine. 1996;124(4):407.
- Motta G, Salzano FA, Motta S, Staibano S. CO2 laser treatment of laryngeal amyloidosis. The Journal of Laryngology & Otology. 2003;117(08).