Introduction
Hepatitis B virus (HBV) infection is an emerging major public health problem globally including in India [
1]. With the high risk of developing chronic HBV infection in 80-90% of newborn and infants when exposed, WHO in 2009 introduced Universal Hepatitis B birth dose (HepB-BD) vaccination soon after birth, preferably within 24 hours, as a key to prevent HBV infection in newborn and infants [
2,
3]. Minimal adverse local reaction such as pain, soreness at injection, and fever after Hepatitis-B birth dose vaccination in newborns are infrequent and transient [3], however injection site abscess is rare. While sterile abscess represents vaccine product-related reactions, pyogenic abscess represents an immunization programme errors [
4].
We report a case of MRSA pyogenic abscess in a four weeks old infant developed after HepB-BD administration. Child was managed surgically followed by appropriate sensitive antibiotic course for three weeks, which results in complete recovery. At follow-up after four months reveal no complications. Various causative factors attributed to the development of post-immunization pyogenic abscess and safe injection practice guidelines are discussed.
Case Report
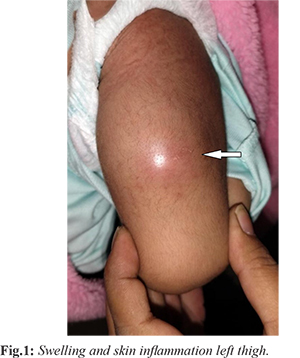
A full-term female neonate was delivered via lower segment cesarean section with a birth weight of 3.5 kg. She received routine immunization, including oral polio vaccine, intradermal Bacillus Calmette-Guérin (BCG) vaccine in the left arm, and Hepatitis B birth dose vaccine administered in the anterolateral aspect of the left thigh at 48 hours of life. One week following vaccination, the mother noticed mild swelling and erythema at the injection site over the left thigh. She consulted a pediatrician, and medications were prescribed. However, due to lack of improvement and progressive increase in swelling, the child was referred to an orthopedician. At presentation to the emergency department at 28 days of age, the infant weighed 4100 g. She was non-toxic, with stable vital signs and a history of low-grade fever for one day. Physical examination revealed a diffuse, tender swelling over the anterolateral aspect of the left mid-thigh with mild fluctuation. The overlying skin was erythematous and indurated [Fig.1], with raised local temperature and reduced active movements of the left lower limb.
Laboratory investigations showed hemoglobin of 11.4 g/dL, total leukocyte count of 17.77 × 109/L with 46% neutrophils, and C-reactive protein of 2.38 mg/L [Table 1]. Radiograph of the left femur demonstrated only soft tissue swelling without any bony involvement [Fig.2]. Based on clinical findings and history, a provisional diagnosis of post-vaccination thigh abscess was made. The infant was admitted and started on appropriate weight-based medical management. However, due to persistent fever and lack of clinical improvement, incision and drainage of the abscess was planned. After obtaining informed consent from the parents, approximately 12 cc of thick purulent material was drained under aseptic conditions in the operating theatre. Thorough wound lavage was performed, and samples were sent for Gram staining and culture sensitivity. No breach of the thigh muscle or periosteum was noted, suggesting superficial localization of the abscess. Pus culture grew methicillin-resistant Staphylococcus aureus (MRSA).
The patient was subsequently treated with oral linezolid at a dose of 30 mg/kg/day for three weeks following discharge. The infant showed complete clinical recovery. At 5 months of age, she demonstrated normal growth and developmental milestones, with no clinical or radiological sequelae [Fig.3,4].
Discussion
WHO recommends Universal Hepatitis B vaccination for all infants at birth and children worldwide [
2]. India has adopted birth dose of Hepatitis B vaccine followed by three doses at 6, 10 and 14 weeks subsequently under Universal Immunization Programme [
4]. The birth dose of 0.5 mL vaccine is administered at 900 angle in vastus lateralis muscle in anterolateral aspect of left thigh intramuscularly through 2-mL syringe with 23G or 25G 25 mm needle [
3]. Hepatitis B vaccine has been considered excellently safe by Global Advisory Committee on Vaccine Safety with mild local pain, myalgia and transient fever as minor adverse reaction following immunization in < 10% children [
2,
4]. Nevertheless, local abscess formation, either sterile or non-sterile, can also develop after vaccination. Injection site abscess represents adverse effect following immunization (AEFI) [
4]. While sterile injection site abscess represents delayed hypersensitivity due to presence of aluminum as an adjuvant or adsorbent used in the vaccines [
5] and is classified as vaccine product-related reactions [
4], a pyogenic abscess at injection site is caused by a breach in skin sterility with subsequent bacterial inoculation at injection site and is classified as immunization error-related reactions [
6], a programme error caused by an error in handling, prescribing and administrating a vaccine [
4].
Injection site abscess following HBV immunization in infants has been a reported AEFI in national immunization programmes and case reports in literature [5,7-9]. A data published on AEFI in children vaccination aged <6 years over 10-years period between 1996 and 2005 by Ministry of Health, Oman reported an incidence of 9.2% injection site abscess (73/790) with 13.7% injection abscess (10/73) following HBV vaccination [
7]. Between 2012 and 2017, Netherlands Pharmacovigilance Centre reported total 40 injection site abscesses with 5 out of 29 (17%) was pyogenic [
5]. Use of improperly sterilized needle and/ or syringe, reuse of disposable needle and/ or syringe, microbial contamination of vaccine using multiple-dose vaccine vial, lack of aseptic measures and unsafe injection practices during vaccine administration is commonly attributed with pyogenic abscess formation [
4,
10]. Most common organism isolated is Staphylococcus aureus, either methicillin-sensitive Staphylococcus aureus (MSSA) or methicillin-resistant Staphylococcus aureus (MRSA) [
6,
9], suggesting common skin commensals to push deep through a skin breach due to negligence in asepsis during intramuscular injections. WHO recommends washing the skin if visibly soiled or dirty, although it recommends no need of skin preparations with 60%-70% alcohol swab prior subcutaneous, intra-dermal and intra-muscular injections including vaccines [
11].
Recently, studies have been conducted on needle size and length for vaccination to ensure appropriate immunological response of vaccines without local side effects. Indian Association of Pediatrics, in accordance with WHO Advisory Committee on Immunization Practices, recommends 23G or 25G needle size for intramuscular vaccination procedures at anterolateral thigh in infants [12]. Lala and Lala proposed 23G over 25G needle as higher gauge needles produce high pressure jet which may cause much trauma [13]. Bierne et al. proposed the use of needles 25 mm in length with 22G to 25G gauge size for intramuscular vaccination of infants [14]. Zukerman proposed long and wide bore needle to ensures deep muscular injection of vaccines for optimum immunogenicity with wider dissipation and low risk of local reaction, inflammation and tissue necrosis post-vaccination [15]. Superficial localization of abscess suggested use of small length of needle in our case and negligence in following WHO recommended safe injection guidelines. Exploiting safe injection practices, use of right needle length and gauge size for optimum vaccine immunogenicity are keystones prior to intramuscular vaccines administration. Any visible skin soiling and dirt must be removed prior intramuscular vaccination. WHO recommends skin disinfection with readily available single use isopropyl alcohol swabs (and not cotton balls) over the site for 30 seconds in spiral motion centrally outward and to wait for further 30 seconds to dry [11]. Health care givers and immunization workers should be trained adequately regarding proper administration of vaccines and injections [4]. Safe injection practices, WHO operational guidelines and SOPs regarding AEFI, use of alcohol-based hand rubs should be taught to health workers through academic workshops. Use of single-dose vaccine vial should be recommended. Rubber stoppers of multiple-dose vaccine vial, a common source of vaccine contamination, should be disinfected with 70% isopropyl alcohol swabs before drawing vaccine [12]. The recommended treatment includes incision and drainage of abscess and appropriate systemic antibiotics.
Conclusion
Pyogenic abscess following Hepatitis B birth dose vaccination is a rare but preventable adverse event, usually related to improper injection technique rather than the vaccine itself. Early diagnosis, drainage, and appropriate antibiotics ensure good outcomes, while strict adherence to safe immunization practices remains essential for prevention.
Contributors: NAQ: manuscript writing, patient management; RPF: manuscript editing, patient management and critical inputs into the manuscript. NAQ will act as study guarantor. Both authors approved the final version of this manuscript and are responsible for all aspects of this study.
Funding: None; Competing interests: None stated.
References
- Technical Guidelines for Diagnosis & management of Hepatitis-B. Ministry of Health and Family Welfare, Government of India. 2019. Available at: Click Here Accessed on August 2, 2025.
- Pattyn J, Hendrickx G, Vorsters A, Van Damme P. Hepatitis B Vaccines. The Journal of Infectious Diseases. 2021;224(Suppl 4):343-351.
- Preventing Perinatal Hepatitis B Virus Transmission: A Guide for Introducing and Strengthening Hepatitis B Birth Dose Vaccination. Click here Accessed on August 2, 2025.
- Adverse effect following Immunization (AEFI): Surveillance and Response Operational Guidelines 2015. Ministry of Health and Family Welfare, Government of India. Click here Accessed on August 2, 2025.
- Injection site abscess after administration of Infarixhexa and synflorix at infant age. [online] Available from: https://www.lareb.nl/Knowledge/FilePreview?id=38445&p=1539. Accessed on August 2, 2025.
- Tan NWH, Pan WJ, Yunos HHBM, Tan WC, Lim KBL. Post-vaccination abscesses requiring surgical drainage in a tertiary children’s hospital in Singapore. J Pediatr Infect Dis. 2010;5(2):139-147.
- Al Awaidy S, Bawikar S, Prakash KP, Al Rawahi B, Mohammed AJ. Surveillance of adverse events following immunization: 10 years’ experience in Oman. East Mediterr Health J. 2010;16(5):474-480.
- Kuyubasi N, Zengin C, Çirakli A, Çirakli S, Kiliç M. Unusual cause of thigh abscess in infant following hepatitis B vaccine administration. J Exp Clin Med. 2013;30(2):181-182.
- Silva L, Lemos S, Cabral J, Alves C. Intramuscular abscess following routine newborn immunization: a case report. J Med Case Rep Case Series. 2022;3(02).
- Chavan S, Vishalakshi P, Vittal DVPR, Rasheeduddin M, Neha, Kondagari D. A case of post-vaccination tubercular abscess in thigh of an infant. J Bacteriol Infec Dis. 2018;2(2):16-18.
- Qamar M, Gillani SW, Azhar S, Sulaiman S. The Skin Preparation Knowledge, Attitudes and Practices among the Healthcare Professionals in Compliance with the World Health Organization (WHO) Guidelines. Journal of Clinical and Diagnostic Research. 2012;6(6):1041-1046.
- Kamath S. IAP Workshop on Safe Injection Practices: Recommendations and IAP Plan of Action. Indian Pediatr. 2005;42(2):155-162.
- Lala KR, Lala MK. Intramuscular Injections: Review and Guidelines. Indian Pediatr. 2003;40(9):835-845.
- Beirne PV, Hennessy S, Cadogan SL, Shiely F, Fitzgerald T, MacLeod F. Needle size for vaccination procedures in children and adolescents. Cochrane Database Syst Rev. 2018;8(8):CD010720.
- Zuckerman JN. The importance of injecting vaccines into muscle. Different patients need different needle sizes. BMJ. 2000;321(7271):1237-1238.