Introduction
Cerebral venous thrombosis (CVT) is an uncommon cerebrovascular disorder and constitutes less than 1% of all stroke cases. Involvement of the deep venous system, referred to as deep cerebral venous thrombosis (DCVT), is particularly rare, representing 11% of CVT presentations [1]. The disease is characterized by a wide spectrum of and often non-specific clinical manifestations, which frequently makes timely diagnosis difficult [2]. Much of the existing knowledge regarding deep CVT has been derived from isolated case reports and limited series, leaving uncertainty in differentiating DCVT from arterial aetiologies when patients present with bilateral thalamic lesions. We considered it important to report this case because bilateral haemorrhagic thalamic infarction is an unusual radiologic presentation in an elderly patient, and recognition of a clearly identified venous cause can significantly alter acute management, diagnostic approach, and prognosis.
Case Report
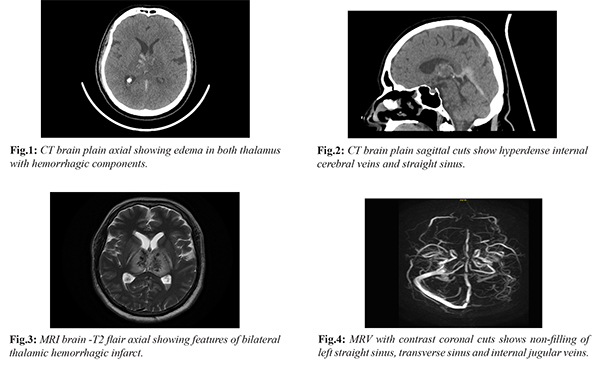
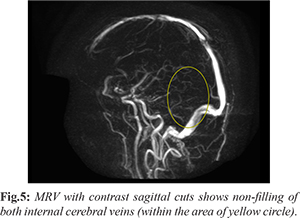
A sixty-one-year-old male with no significant past medical history presented to the emergency department with complaints of headache for two days and sudden onset altered sensorium since the morning of admission. On examination, the patient was drowsy but arousable; he was not communicating and did not obey commands. The pupils were equal in size and reactive to light. He moved both upper and lower limbs spontaneously and showed withdrawal to painful stimuli. Initial computed tomography (CT) of the brain revealed bilateral thalamic haemorrhage with surrounding edema along with a hyperdense straight sinus [Fig.1,2]. The patient was admitted under Neurology with a provisional diagnosis of bilateral thalamic haemorrhagic infarcts secondary to cerebral venous thrombosis. Magnetic resonance imaging of the brain with venography (MRI with MRV) demonstrated thrombosis of the internal cerebral veins, straight sinus, and left transverse sinus [Fig.3,4,5]. Routine haematological and biochemical investigations were within normal limits. Thyroid function tests and thrombophilia work-up, including Factor V Leiden mutation, as well as autoimmune profile were negative. The patient was managed with full-dose enoxaparin and anti-edema measures. During the hospital stay, his sensorium improved; however, he was noted to have developed right-sided hemiplegia. After ten days of treatment, the patient showed marked clinical recovery with residual right hemiparesis. He was able to walk with support and was discharged home in a stable condition.
Discussion
Cerebral venous drainage occurs through two inter-connected pathways: the superficial venous system, which drains cortical brain tissue and comprises the dural sinuses that ultimately empty into the internal jugular vein, and the deep venous system, which is responsible for outflow from midline and deeper structures. The deep system is formed by the paired internal cerebral veins which, along with the basal veins of Rosenthal, unite to create the great cerebral vein of Galen. The straight sinus results from the union of the inferior sagittal sinus and the great cerebral vein [3]. This network drains the thalami, septum pellucidum, basal ganglia, upper brainstem, and the deep white matter of the parietal, temporal, and frontal lobes.
CVT typically manifests with headache, seizures, altered sensorium, and focal deficits such as hemiparesis. In contrast, the presentation of DCVT is frequently non-specific and variable; patients may exhibit transient confusion, speech disturbances, vomiting, convulsions, rapid progression to coma, or even death [4]. Thomas et al., in a study of 32 patients with DCVT, observed that headache and altered sensorium were the most common symptoms [5]. The same study reported that 28% had isolated deep venous thrombosis while the remainder showed involvement of the superficial venous system, and extension beyond the deep system did not influence outcome [5].
MRI with MRV is considered a sensitive modality for detecting both superficial and deep cerebral venous thrombosis. Venous infarction on MRI appears as edema and ischemic changes in structures drained by the deep system, particularly the bilateral thalami, septum pellucidum, basal ganglia, and upper brainstem [4]. However, bilateral thalamic signal abnormalities are not exclusive to DCVT and may also be seen in Japanese encephalitis, Wilson’s disease, Wernicke’s encephalopathy, and hypoxic ischemic encephalopathy [4]. Approximately 22-35% of all thalamic infarcts are bilateral in distribution [6].
Bilateral thalamic infarction can arise from arterial or venous pathology. Most arterial events are related to occlusion of the artery of Percheron, and in a smaller proportion from “top of the basilar” artery thrombosis [4]. Basilar artery thrombosis can usually be distinguished by associated infarcts in the pons or cerebellum in addition to the thalami. Conversely, thrombosis of the internal cerebral veins and straight sinus produces bilateral thalamic venous infarcts. Aetiology of CVT is multifactorial and includes infections, collagen vascular disorders, hypercoagulable states, haematological and hormonal causes, and use of oral contraceptive pills. Studies have described bilateral thalamic infarcts due to venous thrombosis in a patient with ulcerative colitis-related hypercoagulability [7]. Erbguth et al. reported three DCVT patients who achieved excellent recovery with early anticoagulation therapy [8]. Leonard et al., in their review of endovascular management of DCVT, showed that 85% achieved satisfactory recanalization and 62% obtained good functional outcome, recommending that early endovascular intervention be considered in patients presenting with haemorrhagic infarcts [9].
In our patient, thrombosis of the internal cerebral veins and straight sinus accounted for the bilateral thalamic infarction, with additional extension into the superficial venous system. He demonstrated significant recovery with early anticoagulation treatment. Despite extensive laboratory evaluation, no definite underlying cause for venous thrombosis could be identified, underscoring that DCVT may occur even in the absence of recognizable risk factors and that prompt recognition of the venous mechanism is crucial to guide appropriate therapy.
Conclusion
Deep cerebral venous thrombosis is a rare cause of stroke, with evidence largely derived from limited case reports. Differentiating venous from arterial causes of bilateral thalamic infarction is crucial, as management differs fundamentally and venous thrombosis requires prompt anticoagulation. Symmetrical thalamic or basal ganglia lesions have multiple aetiologies, but CVT represents an important and potentially reversible cause. A high index of suspicion, early MRI with MR venography, and timely initiation of appropriate therapy are key to achieving favourable clinical outcomes.
Contributors: AD: manuscript writing and literature search; DNK: manuscript editing; KEA: critical inputs into the manuscript. AD will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study.
Funding: None; Competing interests: None stated.
References
- Gogineni S, Gupta D, Pradeep R, Mehta A, Javali M, Acharya PT, et al. Deep cerebral venous thrombosis-A clinicoradiological study. J Neurosci Rural Pract. 2021;12(3):560-565.
- Kasmaei D, H,Baratloo A, Seddighi AS, Shabani F, Tafreshian M. Galen vein thrombosis with bilateral Thalamus Infarction. Arch Neurosci. 2015;2(2):e19034.
- Tabani H, Tayebi Meybodi A, Benet A. Venous anatomy of the supratentorial compartment. Handb Clin Neurol. 2020;169:55-71.
- Maheshwari S. Cerebral venous thrombosis: An important cause of bilateral thalamic involvement. Acta Scientific Neurology. 2021;4:80-83.
- Pfefferkorn T, Crassard I, Linn J, Dichgans M, Boukobza M, Bousser MG. Clinical features, course and outcome in deep cerebral venous system thrombosis: an analysis of 32 cases. J Neurol. 2009;256(11):1839-1845.
- Sharma S, Dhakal P, Sharma A, Aryal S, Bhandari S, Rajak A. Deep venous sinus thrombosis with right thalamic infarction in a young patient after COVID-19 vaccination. Radiol Case Rep. 2022;17(9):3298-3301.
- Yadav JK, Nepal G, Thapa A, Jaiswal S, Thapa S, Chandra A. Bilateral thalamic infarction following cerebral venous thrombosis in a patient with ulcerative colitis. Clin Case Rep. 2022;10(2):e05404.
- Erbguth F, Brenner P, Schuierer G, Druschky KF, Neundörfer B. Diagnosis and treatment of deep cerebral vein thrombosis. Neurosurg Rev. 1991;14(2):145-148.
- Yeo LL, Lye PP, Yee KW, Cunli Y, Ming TT, Ho AF, et al. Deep cerebral venous thrombosis treatment: Endovascular case using aspiration and review of the various treatment modalities. Clin Neuroradiol. 2020;30(4):661-670.