6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff48d5030000000902000001000a00
6go6ckt5b5idvals|236
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
The peculiar morphologic characteristics of rhinophyma are: teleangectasie, hypervascularity, a thick nasal cutaneous layer, nodularity covered by atrophic skin with expanded pores [
1,
2]. According to these clinical data, El-Azhary classified the rhinophyma in low, moderate, and major degree of disease. The “low” degree of rhinophyma is characterized by telangiectasias and mild skin thickening, the “moderate” by significant thickening of the skin with early formation of lobular areas and the “major” rhinophyma by significant nasal skin hypertrophy and prominent nodular enlargement. If it is left untreated can result in distortion of soft tissue and airway obstruction [
2,
3].
Though rare in occurrence, malignant tumors can grow over rhinophymatous skin, with BCC being the most commonly reported tumor (38 cases). Wende and Benz first reported coexisting carcinomas with rhinophyma in 1904 and subsequently sporadic reports were published but for the few data in literature, cannot be determined if there is an etiopathogenetic or incidental correlation [
1-
7].
Case Reports
We report four cases of BCC arising on rhinophyma observed between 1998 and 2012 at the Plastic and Reconstructive Unit, Department of Surgical Oncologic and Sthomatologic Sciences, University of Palermo.
In our cases, BCC arise on rhinophyma with nodular, nodular-crusted or crusted-ulcer clinic types. All patients were male with ages between 64 and 80 years. Three patients had a low degree and one patient had major degree of rhinophyma according to El-Azhary classification. Two patients had history of skin cancer in the face and alcoholism with long-standing rhinophyma. There were no enlarged regional lymph nodes. Biopsy of atypical lesions and decortications was done in all cases with histologic confirmation.
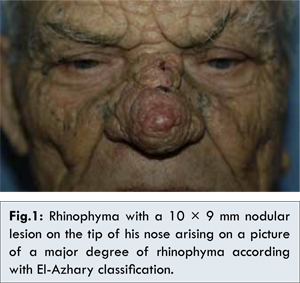
Case 1: A 80 year old man presented for excision of his major degree of rhinophyma, according with El-Azhary classification, of 14-year duration. He was non-smoker and nonalcoholic, with no history of cancers in the face. A careful examination of the nose, revealed the presences of an atypical nodular lesion on the tip with 10x9 mm size. This lesion was pinkish-purple in color, with hard consistency, smooth and poorly defined edges. On the back of the nose were also two small crusted areas. Nodular lesions, typical of rhinophyma, were present on the whole skin of the nose with different clinical features: light-brown color, hard elastic consistency and defined edges. There was no lymphadenopathy or similar lesions in other parts of his face. Under general anesthesia, we performed biopsies of these lesionsand decortications by scalpel of all aesthetic units of the nose and autologous skin graft. The histological examination showed a nodular type BCC for the nodular lesions and superficial BCC for the crusted areas [Fig. 1].
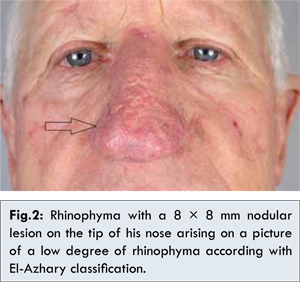
Case 2: A 64 year old man presented with a 2 year history of long-standing rosacea resulting in a low degree of rhinophyma and a nodular lesion on the tip of his nose with 8x8 mm size. The patient was smoker and alcoholic without any history of cancers in the face. This lesion was pinkish-purple in color, with hard consistency, smooth and poorly defined edges. ETG exam not showed loco regional enlarged lymph nodes. No similar lesions were present in the face. Biopsy of the nodular lesion and reconstruction with autologous skin graft was performed under local anaesthesia. The histological examination confirmed clinical diagnosis of nodular type BCC. The rhinophyma was subsequently treated with medical therapy (Metronidazole and isotretinoin) [Fig. 2].
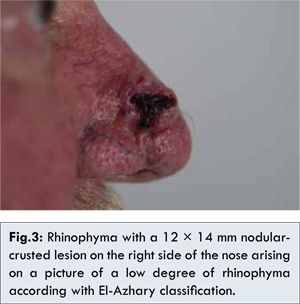
Case 3: A 70 year old man comes to our attention for a nodular-crusted lesion on the right side of the nose with 12x14 mm in size, present for four years, arising on alow degree of rhinophyma of 10 year duration. The patient had a history of smoking and alcoholism and no history of cancer in the face. This lesion was nodular with a central crust, hard consistency and poorly defined edges. There were no enlarged regional lymph nodes or similar lesions in other parts of his face. Biopsy of the nodular lesion and reconstruction with autologous skin graft was performed under local anaesthesia. The histological examination confirmed the clinical suspected of nodular ulcer BCC. Medical therapy of rhinophyma was subsequently conducted [Fig. 3].
Case 4: A 75 year-old man who was a non-smoker and nonalcoholic, presented with a painless and non-healing ulcer on the dorsum of his nose, present for two years. On a careful examination this lesion was of 18x16 mm in size with pearly beaded edges and the nose showed a picture of a low degree of rhinophyma of 10 year duration. There were no enlarged regional lymph nodes or similar lesions in other parts of his face. Histological examination showed a nodular ulcer BCC. Reconstruction was performed with autologous skin graft under local anesthesia. Medical therapy was conducted for therhinophyma [Fig. 4].
Discussion
Rhynophyma is a nose hypertrophy condition that is considered the end stage of acne rosacea. In literature a wide range of surgical approaches to rhinophyma has been described such as dermo-abrasion, scalpel shave, cryosurgery, electrocautery, near total excision with skin grafting, and laser excision.
The rhinophyma can hide among its typical clinical signs a BCC and other malignancies. The coincidence of BCC with rhinophyma is well-known but for the few data in the literature the data incidence varies. In a review published in 1998, Baruchin reported that, since 1955, only 32 cases of BCC on rhinophyma [
2].
In 1967 Acker and Helwig, through a retrospective study of 47 patients with rhinophyma, found the presence of associated malignant lesions in seven patients. In five cases there was association with BCC, in one case there was association with squamous cell carcinoma and in one with sebaceous adenoma. The incidence of occult BCC was higher in patients with rhinophyma than with free nasal skin [
8]. Subsequent work of literature review conducted by Keefe disproves the hypothesisof a pathogenetic association between rhinophyma and BCC because itis not sufficient the only evidence of this association and could be a coincidental event [
9].
Brubaker and Hellstrom identified the area of carcinomatous change to be the papillary buds emanating from the basal layer of the dilated follicles. These authors postulated that BCC will develop in more than 5% of patients with rhinophyma [
10]. Wende and Bentz reported a patient with rhinophyma in whom histological examination revealed five different tumors [
11]. Novick and Acker postulated that the fibrous scarring frequently present in rhinophyma orthat the hyperplasia and hypertrophy influences the overlying epidermis towards malignant degeneration [
12,
13]. Elliott and Al. concluded that although the presence of BCC may be difficult to diagnose clinically, its presence may be histologically detected in 3-10 percent of rhinophyma cases [
14].
This suggests that although a rare event, the development of BCC should always be sought in presence of rhinophyma, especially when arising since years (whether this is a true association remains unclear) and also small changes of the skin lesion, characteristic that it represents. The presence of a clinical aspect change of the rhinophyma, with arising secretion, ulceration, nodular size variation after years of quiescence must place the suspected diagnosis. Owing to the few data in literature, etiopathogenetic or incidental correlation between BCC and rhinophyma is difficult to determine.
Conclusion
We report four new cases of BCC arising on rhinophyma. It is suggested that special attention to be paid to local objective examination of patients with rhinophyma and to all those lesions that could conceal the presence of this cancer. A small lesion may be the ‘tip of the iceberg, and biopsy should be performed of all suspected lesions. Histological confirmation of the clinical suspicion needs a close follow-up.
References
- Leyngold M, Leyngold L, Letourneau PR, Zamboni WA, Shah H. Basal cell carcinoma and rhinophyma. Ann Plast Surg. 2008;61:410-412.
- Baruchin AM, Nahlieli O, Shapira Y, Ben-Dor B, Rosemberg L. Surgical treatment of rhinophyma associated with basal cell carcinoma: report of four cases. Eur J Plast Surg. 1998;21:374-377.
- Bogetti P, Boltri M, Spagnoli G, Dolcet M. Surgical Treatment of Rhinophyma: A Comparison of Techniques. Aesth Plast Surg. 2002;60:26-57.
- Lutz ME, Otley CC. Rhinophyma and Coexisting Occult Skin Cancer. Dermatol Surg. 2001;27:201-202.
- Lazzeri D, Agostini T, Pantaloni M, Spinelli G. Rhinophyma and non-melanoma skin cancer: an update. Ann Chir Plast Esthet. 2012;57:183-184.
- Qassemyar A, Corbisier N, Poiret G, Mortier L, Martinot-Duquennoy V, Guerreschi P. Rhinophyma and skin carcinoma: a case report and litterature review. Ann Chir Plast Esthet. 2012;57:169-172.
- Lazzeri D, Colizzi L, Licata G,Pagnini D, Proietti A, Alì G. Malignancies within rhinophyma: report of three new cases and review of the literature. Aesthetic Plast Surg. 2012; 36:396-405.
- Acker DW, Helwing EB. Rhinophyma with carcinoma. Arch Dermatol. 1967;195:250-254.
- Keef M, Wakeel RA, McBride DI. Basal cell carcinoma mimicking rhinophyma. Case report and literature review. Arch Dermatol. 1988;124:1077-1079.
- Brubaker DB, Hellstrom RH. Carcinoma occurring in rhinophymas. Arch Dermatol. 1977;113:847-848.
- Wend GW, Bentz A. Rhinophyma: a pathological analysis of five separate tumours occurring in the same patient. J Cutan Dis. 1904;22:447-460.
- Novick NL, Kest E, Gordon M. Advances in the biology of and carcinogenesis of basal cell carcinoma. NY State J Med. 1988;88:367-370.
- Acker DW, Helwing EB. Rhinophyma with carcinoma. Arch Dermatol.1967;195:250-254.
- Elliot RA, Ruff LE. Rhinophyma and its treatment. ClinPlast Surg. 1980;7:277-288.