|
|
|
|
|
Middle Cerebral Artery Dissection Presenting with Intracerebral and Subarachnoid Hemorrhage
|
|
|
|
Tony Ete, Sumantro Mondal, Debanjali Sinha, Soumik Sarkar, Kaushik Bhar, Sattik Siddhanta, Jyotirmoy Pal, Alakendu Ghosh
From the Department of Medicine, Institute of Post Graduate Medical Education and Research, Kolkata, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr. Tony Ete
Email: tetepete@gmail.com |
|
|
|
|
|
|
|
|
Received:
08-NOV-2013 |
Accepted:
03-DEC-2013 |
Published Online:
10-DEC-2013 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Dissecting aneurysm of the intracranial arteries is uncommon and isolated dissection of middle cerebral artery (MCA) is much rarer. Cerebral infarction is the usual presentation of MCA dissection in first two decades, hemorrhagic manifestation being much rare. We describe a young male patient who presented with acute onset headache and left sided hemiparesis due to acute intra-parenchymal hemorrhage. Digital subtraction angiography finally revealed dissection involving M2 segment of right MCA as the possible cause of intracerebral hemorrhage in this patient. This type of uncommon presentation of MCA dissection is rarely reported before. |
|
|
|
|
|
Keywords :
|
Middle Cerebral Artery, Cerebral Hemorrhage, Aneurysm, Paresis, Stroke, Headache.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffd8b7040000007b02000001000d00 6go6ckt5b5idvals|269 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Stroke in a young has an increasing incidence now a days. Hemorrhagic stroke in younger population has varied etiologies. Dissecting aneurysm of middle cerebral artery (MCA) is not so common. It commonly manifests as cerebral ischemia and hemorrhage is rather rare. MCA aneurysm rupture and re-rupture has got a high mortality rate of more than 60% within 2 years [ 1, 2]. Our patient, a non-hypertensive teen aged male presented with acute intraparenchymal and minimal sub-arachnoid hemorrhage and finally diagnosed as having dissection of MCA by angiography.
Case Report
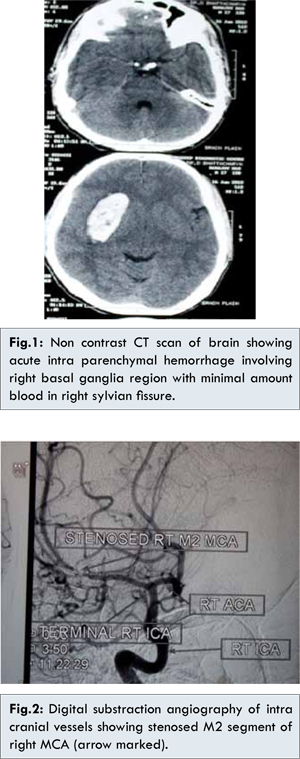
A 17 years old non diabetic, non-hypertensive male presented in the emergency department with a history of acute onset severe headache followed by weakness of left side of body for the last two days. There was no history of loss of consciousness, episodes of seizure or vomiting. The patient had no history of drug addiction, trauma or any history suggestive of bleeding disorder. There was no similar history in family. The patient had normal developmental milestones. On examination higher mental functions were normal. Pulse was 76/minute and blood pressure was 122/78 mmHg.Neck rigidity was present. Tone of both upper and lower limbs was diminished in the left half of the body. Power of upper and lower limbs were normal on right side however power in left upper and lower limb were reduced (MRC grade 2/5). Deep tendon jerks were diminished on left half of the body. Plantar response was extensor on left side. No cranial nerve involvement was present. No abnormality was detected in the cardiovascular and other systems. Plain CT scan of brain revealed acute intracranial hemorrhage (ICH) in right basal ganglia with minimal amount of blood in the right sylvian fissure [Fig.1]. Routine blood investigations including hemoglobin, total leucocyte count, platelet count, random blood sugar, lipid profile, liver function and renal function tests were within normal limit. Blood for prothrombin time, protein C, protein S, Factor V Leiden mutation, homocysteine levels were also evaluated and found to be within normal range. CSF study done on fifth day of admission was normal. Echocardiography was normal. MRI study of the brain was also corroborative with CT scan finding and it showed hematoma in the right basal ganglia region. The patient underwent Digital subtraction angiography of both carotid artery and the report revealed stenosis of M2 segment of right middle cerebral artery indicating healed dissecting aneurysm of middle cerebral artery (MCA) [Fig.2]. The final diagnosis was dissection of right MCA with acute intracerebral hemorrhage in right basal ganglia with minimal sub-arachnoid hemorrhage. The patient was referred to department of neurosurgery for further management.
Discussion
Dissection of cervical or cephalic arteries is not much common. Isolated dissection of MCA is even rarer. There is paucity of data regarding the actual incidence of MCA aneurysmal dissection.According to Japanese study, the incidence of MCA dissection could be up to 4% of the spontaneous cervico-cephalic dissections [ 3]. MCA dissection has been sub classified into two categories: (i) Isolated dissection of MCA and (ii) Extended dissection from distal portion of internal carotid artery. Isolated MCA dissection is a rare entity and its etiologies, clinical manifestations, natural history and prognosis remain poorly understood. Isolated MCA dissection is associated with more fluctuating course [ 4].It may present with localized warning symptoms ipsilateral to the diseased vessel in the form of pain in the head or neck and disturbed sympathetic activity of the face [ 5]. The headache sometimes may be as severe as sub-arachnoid hemorrhage. Transient monocular blindness or ischemic attacks may also be present. Sometimes the aneurysm is detected accidentally without any symptom. In younger population cerebral infarct is the common manifestation of MCA dissection [ 6]. Even on long term follow up there is very rare chance of the patients developing intracranial bleeding after the ischemic onset [ 7]. This is notable because our patient developed hemorrhagic manifestation of MCA dissection at an earlier age which is very rare.
ICH in a non-hypertensive young patient is commonly caused by trauma, drug abuse, coagulation disorders, aneurysm and cerebral arterio-venous malformation. All these conditions were the possible differential diagnostic consideration in our patient. These possibilities were ruled out in our patient by relevant investigations. Finally DSA documented the presence of MCA dissection as the causative factor for ICH in our patient. Though uncommon, hemorrhagic manifestations can be encountered in MCA dissection. Few recent reports documented that MCA dissection may be associated with sub arachnoid hemorrhage (SAH). Rupture of bacterial aneurysm causing SAH has been reported from Japan [8]. In bacterial aneurysm local inflammation causes weakness of vessel wall with resulting rupture of dissection [ 8]. False lumen is represented by the ectatic components of the arterial dissection and persistent aneurysmal dilatation of the vessel might indicate destruction of elastic or lamina muscularis leading to increase in the potential risk of bleeding [ 9]. However, in our patient DSA did not show any evidence of MCA ectasia and neither there was any clinical evidence of infection. Cases of dissecting MCA aneurysm causing intracerebral hemorrhage years after the non-hemorrhagic onset have been reported [ 10, 11]. In the contrary, our patient presented with acute onset headache with focal neurological signs and neuroimaging study confirmed the presence of acute ICH. It can be concluded that ICH was the initial manifestation of MCA dissection in him. We report this case as an example of rarer presentation of an uncommon entity.
Conclusion
Dissection of MCA rarely causes hemorrhagic manifestation even in young. In the absence of other common causes of ICH in a young, dissection should be a diagnostic consideration and angiography of intracranial arteries can be very informative.
References
- Choi IS, David C. Giant intracranial aneurysms: development, clinical presentation and treatment. Eur J Radiol. 2003;46:178–194.
- Drake CG, Peerless SJ. Giant fusiform intracranial aneurysms: review of 120 patients treated surgically from 1965 to 1992. J Neurosurg.1997;87:141–162.
- Tsukahara T, Minematsu K. Overview of spontaneous cervicocephalic arterial dissection in Japan. Acta Neurochir Suppl. 2010;107:35–40.
- Lee JS, Bang OY, Lee PH, et al. Two case of spontaneous middle cerebral arterial dissection causing ischemic stroke. J Neurol Sci. 2006;205:162-166.
- Liu YC, Chung CP, Yip PK, Wang V. Spontaneous middle cerebral arterial dissection presented with limb shaking. Acta Neurol Taiwan. 2009;18(1):26-29.
- Ohkuma H, Suzuki S, Shimamura N, Nakano T. Dissecting aneurysms of the middle cerebral artery: neuroradiological and clinical features. Neuroradiology. 2003;45(3):143-148.
- Abiko S, Okamura T, Kurokawa Y, Ikeda N, Ideguchi M, Watanabe K. Diagnosis and treatment of nontraumatic dissecting aneurysm in the middle cerebral artery. No Shinkei Geka. 1999;27:743–749.
- Saito A, Kawaguchi T, Hori E, Kanamori M, Nishimura S, Sannohe S, et al. Subarachnoid Hemorrhage After an Ischemic Attack Due to a Bacterial Middle Cerebral Artery Dissecting Aneurysm: Case Report and Literature Review. Neurol Med Chir (Tokyo). 2013; Oct 21. PMID: 24140774.
- Kitanaka C, Tanaki J, Kuwahara M, Teraoka A, SasakiT, Takakura K. Nonsurgical treatment of unrupture intracranial vertebral artery dissection with serial follow-up angiography. J Neurosurg. 1994;80:667–674.
- Isono M, Abe T, Goda M, Ishii K, Kobayashi H. Middle cerebral artery dissecting aneurysm causing intracerebral hemorrhage 4 years after the non-hemorrhagic onset: a case report. Surg Neurol. 2002;57(5):346-350.
- Joshua SA, Nayak SG, Pare VS, Ashok, Sebastian R. Unruptured Intracranial Aneurysm Involving the Distal Anterior Cerebral Artery: A Cadaveric Study. Journal of Case Reports. 2013;3(1):5-9.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Ete T, Mondal S, Sinha D, Sarkar S, Bhar K, Siddhanta S, Pal J, Ghosh AMiddle Cerebral Artery Dissection Presenting with Intracerebral and Subarachnoid Hemorrhage.JCR 2013;3:451-454 |
|
Ete T, Mondal S, Sinha D, Sarkar S, Bhar K, Siddhanta S, Pal J, Ghosh AMiddle Cerebral Artery Dissection Presenting with Intracerebral and Subarachnoid Hemorrhage.JCR [serial online] 2013[cited 2026 Jun 6];3:451-454. Available from: https://www.casereports.in/articles/3/2/Middle-Cerebral-Artery-Dissection-Presenting-with-Intracerebral-and-Subarachnoid-Hemorrhage.html |

|
|
|
|
|