6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff342b040000002c02000001000800
6go6ckt5b5idvals|249
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Hydatidosis (Echinococcosis) is caused by the larval stage of Echinococcosis granulosus, which remains endemic in many countries of the world [
1]. Hydatid cyst of liver is common while pancreatic hydatid cyst is rare, even in endemic countries. The reported incidence varies from 0.19% to 2% of patients with hydatid disease [
2]. Treatment of hydatid cyst can be difficult when it involves pancreas. We present a case of large pancreatic hydatid cyst along with two calcified liver hydatid cyst managed successfully with surgery.
Case Report
A 26 year old male patient presented with complaints of non radiating pain in left side of abdomen with no aggravating & relieving factors. General physical examination was within normal limits. Abdominal examination revealed a non-tender lump palpable in left hypochondric region of size 5×5 cms, along with hepatomegaly. Routine investigations revealed hemoglobin 12.3 gm/dl, total WBC count 4500/mm3 with DLC showing raised eosinophil count (9%). Liver function test, serum amylase and lipase were within normal limits.
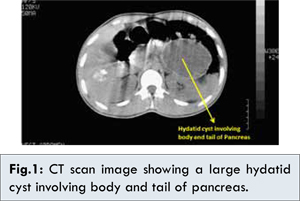
X ray chest did not reveal any abnormality. Ultrasound abdomen showed a hydatid cyst measuring 8×6 cms in size close to pancreatic tail region extending infero-laterally and two small isoechoic calcified hydatid cysts in right lobe of liver. CT scan abdomen revealed well defined fluid attenuation non-enhancing lesion in the body and tail region of pancreas of size 8.9x6.6 cms, suggesting hydatid cyst in pancreas. Two calcified hydatid cyst of sizes 3.3x3.1 cms and 3.1x2.9 cms in segment 5 and 6 of the liver respectively [Fig.1].
Patient was given pneumococcal, H.Influenzae and menningococal vaccine pre-operatively in view of possibility of splenectomy. Explorative laparotomy revealed one large cyst involving body and tail of pancreas and two cysts in liver. Cystopericystectomy was done for the two cysts in liver. While pancreatic cyst was first aspirated, this revealed clear watery fluid. The cyst was opened and the diagnosis of hydatid cyst was confirmed by presence of laminated membrane and daughter cysts. In view of possible communication with pancreatic duct due to large size of the cyst, roux en-Y cysto-jejunostomy was done [Fig.2-5]. Post operatively patient recovered well. Tablet albendazole 400 mg once a day was started from 5th postoperative day for a period of three months. Patient is on follow up for more than 4 years now without any symptoms or recurrence.
Discussion
Hydatid cyst occurs commonly in liver and lung but pancreatic hydatid cyst has been rarely reported. The location of the cyst in the pancreas has different distributions: head (57%), corpus (24%) and tail (19%) [
3]. Clinical presentation is variable and insidious, depending on the location and the size of the cyst [
4]. Epigastric pain is the most frequent symptom [
5]. Our patient presented with pain in left hypochondriac region, but abdominal examination revealed an abdominal lump. Cysts in the corpus and tail rarely cause any symptoms and abdominal mass may be found on examination.
The diagnosis of pancreatic cystic lesion may be performed by ultrasonography, CT scan or MRI. Various immunological tests are also available to confirm the diagnosis of hydatid cyst when there is doubt. In our case diagnosis was confirmed on ultrasound and CT scan hence no immunological tests were done.
Chemotherapy is effective in small cyst with diameter less than 4 cm, those with thin walls and in younger patients. It is also indicated in patients who are at high risk for surgery, in patients with multiple peritoneal cysts, cysts in multiple organs, bone cyst, cyst in brain, to prevent secondary echinococcosis after spillage during surgery and as a concomitant therapy with percutaneous drainage [
6]. Albendazole (10 mg/kg/day) is the most common drug used in medical treatment of hydatid cyst. Used before and after surgery, or only after surgery seems to be efficient, as the appearance of the recurrences is absent [
7]. This justifies our decision of prescribing tablet albendazole to the patient in the post-operative period. The drug penetrates hydatid cyst and act by blocking glucose uptake in the parasite and depletion of its glycogen stores.
Regardless of its location, hydatid cyst is best cured surgically. In pancreatic disease, it’s essential to maintain the organ’s exocrine and endocrine functions. Many surgical techniques are available to remove the cyst; however pericystectomy with drainage of the residual cavity is the technique of choice [
4,
8]. Because of the localization of the cyst near a major biliary or vascular structures and high risk of pancreatic fistula [
9], total pericystectomy cannot be done in some cases. Open cyst evacuation and omentopexy can be done in these cases when there is no communication with pancreatic duct.
If communication between the cyst and the pancreatic duct is suspected, internal drainage like cysto-gastrostomy, roux-en-Y cysto-jejunostomy should be done to prevent pancreatic fistula. In our case, size of cyst was large hence we suspected communication with pancreatic duct and did internal drainage as this appeared to be the safest option.Distal pancreatectomy with splenic conservation is the treatment of choice for hydatid cyst localized in the tail of pancreas [
4]. Percutaneous treatment of pancreatic hydatid cyst using catheter technique has also been reported in few properly selected cases [
10].
Conclusion
Management of cyst cavity after evacuation of hydatid cyst is a major issue. It becomes critical when there is involvement of important organ like pancreas, where organ has to be preserved and there is a possibility of communication with pancreatic duct. This case presents a successful method of dealing with this issue by roux-en-Y cystojejunostomy.
References:
- Bouree P. Hydatidosis: dynamics of transmission. World J Surg. 2001;25:4-9.
- Khiari A, Mzali R, Ouali M, Kharrat M, Kechaou MS, Beyrouti MI. Hydatid cyst of pancreas. Apropos of 7 cases. Ann Gastroenterol Hepatol. 1994;30:87-91.
- Gayral F, Bourree P, Jourdanne PH, Millat B, Labayle D. Hydatid cyst of the pancreas. Nouv Presse Med. 1981;10:3787-3788.
- Arikan A, Sayan A, Erikci VS. Hydatid Cyst of pancreas: A case report with 5 years follow up. Pediatr Surg Int. 1999;15:579-581.
- Fadil A, Bolbarod AA, el Fares F. Hydatid cyst of the pancreas. Report of a case. Ann Chir. 2000;125:173-175.
- Khuroo MS. Hydatid disease: Current status and recent advances. Ann Saudi Med. 2002;22:56-64.
- Radulescu S, Angelescu N, Horvat T, Lazar L, Creau C, Popa L, et al. Clinical study of efficacy of albendazole treatment in human hydatidosis. Chirurgia (Bucur) 1997;92:331-335.
- Faucompret S, Farthouat P, Sainton T, Breda Y. Complicated hydatid cyst of the pancreas after needle biopsy. Ann Chir. 2001;126:491-492.
- Achour A, Daali M. Kystehydatique du pancrias. J Chir. 2005;142:331-332.
- Karaman B, Battal B, Ustunsoz B, Ugurel MS. Percutaneous treatment of primary pancreatic hydatid cyst using a catheter technique. Korean J Radiol. 2012;13:232-236.