6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff1454050000007102000001000800
6go6ckt5b5idvals|290
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
A coronary artery ?stula (CAF) is an abnormal connection between a coronary artery and a cardiac chamber, a great vessel or any other vascular structures. Although most coronary artery anomalies do not cause myocardial ischemia and are diagnosed incidentally, some of these anomalies may cause angina, myocardial infarction or sudden death. We report the two incidental founded cases of coronary-to-pulmonary artery fistulas who presented with acute coronary syndrome.
Case Reports
Case 1
A 59 year-old man admitted to our emergency unit with complaint of chest pain. The patient’s consciousness suddenly deteriorated and emergency unit staff recognized ventricular fibrillation on the ECG. After emergency defibrillation his ECG had revealed ST segment elevations in DII, DIII and AVF leads confirming the diagnosis of acute inferior MI. After then he was sent to our catheterization unit for further therapeutic evaluation. His cardiovascular risc factors were smoking and hypertension. His blood pressure and heart rate were 100/60 mmHg, 82 bpm, respectively. Physical examination was normal.
Transthoracic echocardiography showed inferior and lateral wall hypokinesia of left ventricle, mild mitral regurgitation and mild systolic dysfunction (left ventricular ejection fraction was 45%). Pulmonary artery systolic pressure was measured as 35 mmHg by using tricuspid regurgitant jet velocity. Coronary angiography showed a coronary artery fistula originating from the left anterior descending (LAD) artery and draining into the left pulmonary artery [Fig.1]. A total occlusion of the left circumflex coronary artery (Cx) in the mid portion was detected and a bare metal stent was implanted, successfully. Since the patient was clinically stable, he was discharged on the fifth day of admission. We performed myocardial perfusion scintigraphy and founded normal myocardial perfusion at anterior region of the heart. The patient is now asymptomatic and in the follow up list for three years.
Case 2
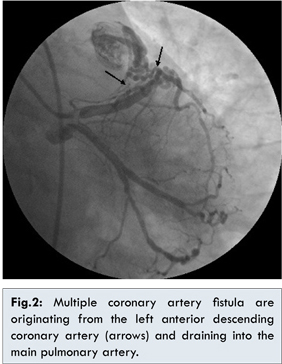
A 67 year-old woman admitted to our department with exercise induced angina for two days. She had no history of cardiac disease or trauma and her physical examination was normal. The 12-lead electrocardiogram revealed T wave inversion in leads DII, DIII, AVF. Transthoracic echocardiography showed inferior wall hypokinesia of left ventricle, mild mitral regurgitation and mild systolic dysfunction (left ventricular ejection fraction was 43%). Pulmonary artery systolic pressure measured 40 mmHg by using tricuspid regurgitant jet velocity. Selective angiography of the right coronary artery demonstrated 95% stenosis at mid-portion, as well as a 70% narrowing at the ostium. Selective angiography of the left coronary system demonstrated multiple coronary artery fistulas originating from the left anterior descending (LAD) artery and draining into the main pulmonary artery [Fig. 2]. The circumflex artery was narrowed by 70% distally near the 2nd obtuse marginal branch. Because of her anginal symptoms, multiple coronary artery fistulas and two vessel diseases, coronary artery bypass surgery with surgial closure of the fistulas was recommended and transferred to cardiovascular surgery clinic for operation.
Discussion
The incidence of coronary-to-pulmonary artery fistula in coronary angiograms has been reported to be 0.2% [
1]. Coronary-to-pulmonary artery ?stulas originated from the right coronary artery are 15% of cases, from the left coronary artery are 53%, from both coronary arteries are 7%, from a single coronary artery is 7%, and unknown is 13% [
2]. The coronary-to-pulmonary fistulas are usually discovered incidentally during routine cardiac catheterization after development of coronary artery disease, as in our cases. They are mostly asymptomatic and present without an audible murmur. In our cases, there was not any audible murmur or another sign in physical examination.
The etiology of fistulas are classified as acquired (e.g., trauma, infection, neoplasm and surgery) or congenital. Our patients had no history of any disease or trauma that could have led to such fistulas. A great majority of the coronary-pulmonary fistulas in adults, whether congenital or acquired, are benign, in terms of their effect on coronary physiology [
3]. Surgical or percutaneous closure of the fistula is recommended if it causes myocardial ischemia, large left-to-right shunts, and heart failure [
4]. When symptomatic, coronary artery fistulas are associated with poor outcomes, and in order to prevent complications, closure is recommended at all ages [
5]. Several authors recommended that intervention was necessary for asymptomatic patients because their natural course is unknown [
6].
The selection of therapeutic option is controversial. Recently, transcatheter closure of coronary artery fistula has been reported as an acceptable alternative to surgery. However, the anatomy and characteristics of some fistulas do not allow catheter intervention. Because our second case has anginal symptoms, multiple coronary artery fistulas and two vessel diseases, coronary artery bypass surgery with surgial closure of the fistulas was chosen for this patient therapy. In our first case, fistulas were considered asymtomatic, because the patient presented with acute myocardial infarction with no apparent relation to his coronary-to-pulmonary artery fistulas. He was started on medical treatment since his myocardial perfusion scintigraphy also showed normal perfusion of anterior myocardial region. Different authors reporting on follow-up of such asymtomatic patients recommended different strategies, from elective closure irrespective of symptoms, especially in childhood, to conservative management, particularly in presence of small fistulas, which is most often the case when they drain into the pulmonary trunk [
7]. Now the patient is asymptomatic and in the follow up list for three years.
The selection of therapeutic option is controversial. If the fistulas are small or does not cause ischemia follow up can be the alternative strategy. If ischemia occurs secondary to fistula or is symptomatic, trans-catheter closure of coronary artery fistula or surgery can be the choice for treatment. In appropriate cases, trans-catheter closure can be the alternative to surgery. However, surgical repair may be indicated in cases of coronary artery fistulas with additional complex heart disease which requires surgery.
References
- Urrutia-S CO, Falaschi G, Ott DA, Cooley DA. Surgical management of 56 patients with congenital coronary artery fistulas. Ann Thorac Surg. 1983;35:300-307.
- Furushima Y, Kasuya S, Murota K, Matsuzawa H. Congenital coronary artery fistula. Compilation and evaluation of cases reported in Japan. Nippon Kyobu Geka Gakkai Zasshi. 1976;24:1409-1419.
- Bhandari S, Kanojia A, Kasliwal RR. Coronary artery fistulae without audible murmur in adults. Cardivasc Interv Radiol. 1993;16:219-223.
- Hoffer E, Materne P, Henroteaux D, Markow M, Boland J. Succesful percutaneous closure of multiple coronary artery fistulas with coils embolization in two adults. Int L Cardiol. 2007;122:25-28.
- Balanescu S, Sangiorgi G, Lee JD, Castelvecchio S, Medda M, Inglese L . Coronary artery fistulas: Clinical consequences and methods of closure. A literature rewiew. Ital Heart J. 2001;2:669-676.
- Yamada Y, Imamura H, Amamoto Y, Ochi M, Nagono K, et al. Congenital internal mammary artery-to-pulmonary artery fistulas: A Case Report. Heart Vessels. 1987;3:47-49.
- Armsby LR, Keane JF, Sherwood MC, Forbess JM, Perry SB, Lock JE. Management of coronary artery fistulae. Patient selection and results of transcatheter closure. J Am Coll Cardiol. 2002;39:1026-1032.