|
|
|
|
|
OPG and CBCT Finding’s of an Ectopic Third Molar in the Sub-condylar Region
|
|
|
prednisolon prednisolon kur link
From the Department of Oral Medicine and Radiology1, Sree Mookambika Institute of Dental Sciences, Kulasekharam, Kanyakumari District, Tamilnadu; Department of Public Health Dentistry2, Annoor Dental College, Muvattupuzha, Kerala, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Farakath Khan
Email: farakath@gmail.com
|
|
|
|
|
|
|
|
|
Received:
11-JUN-2014 |
Accepted:
01-JUL-2014 |
Published Online:
05-AUG-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Impaction of third molar is a common developmental abnormality. However, ectopic impaction of the mandibular third molar in subcondylar region is an extremely rare condition. This report describes a case of impacted tooth in the subcondylar region without any associated pathologic condition and it’s spatial relationship to the surrounding anatomic structures using cone beam computed tomography. |
|
|
|
|
|
Keywords :
|
Third molar, Impacted tooth, Tooth Eruption, Molar, Mandible, Unerupted Tooth.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa0e8050000000e03000001000800 6go6ckt5b5idvals|349 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Impaction of a tooth is a situation in which an unerupted tooth is wedged against another tooth (or teeth) or otherwise located so that it cannot erupt normally [1]. The mandibular third molar is the most frequently impacted tooth. Impacted mandibular third molars are categorized according to the anterior posterior space between the second molar and the mandibular ramus, its medial lateral position in the body of the mandible, and the position of its long axis. Ectopic mandibular third molars, however, are rare and usually diagnosed from clinical symptoms. The reason as to why third molars are sometimes ectopically placed is unknown. However, trauma, aberrant eruption and anomalous development of the tooth germ are all theories that have been postulated.
Their heterotrophic positions were reported to be in the condylar area, in the ascending ramus of the mandible, or in the coronoid process [2]. Unilateral or bilateral ectopic impacted third molar teeth have been reported in various parts of the mandibular ramus. This report presents an ectopic mandibular third molar in the mandibular subcondyle without any pathologic condition.
Case Report
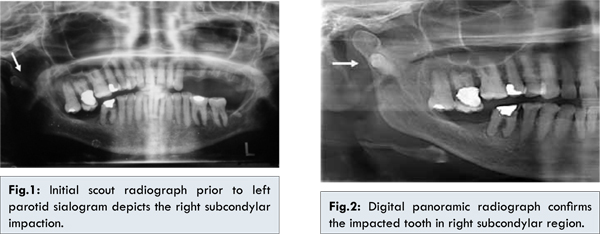
A 60 year old female reported to clinic with the chief complaint of pain in left parotid region. Patient gives history of chronic pain since 2 years and prolonged history of occasional discomfort since early forties. She consulted a host of specialties and was diagnosed as chronic bacterial sialadenitis. Panoramic radiograph showed generalized alveolar bone destruction. All the teeth showed moderate attrition. Deep restorations were present in 14, 17, 36, 46 with periapical lesions. 24, 25, 26, 27, 28, 38, 47, 48 were missing. History suggested extraction of 47 long back, and conclusively a history of nonextraction of the 48. Incidentally, a well formed, impacted tooth was found in the right subcondylar region of the mandible. The tooth crown seemed directed into the head of the condyle [Fig.1], the digital OPG that was taken [Fig.2] confirmed the same.
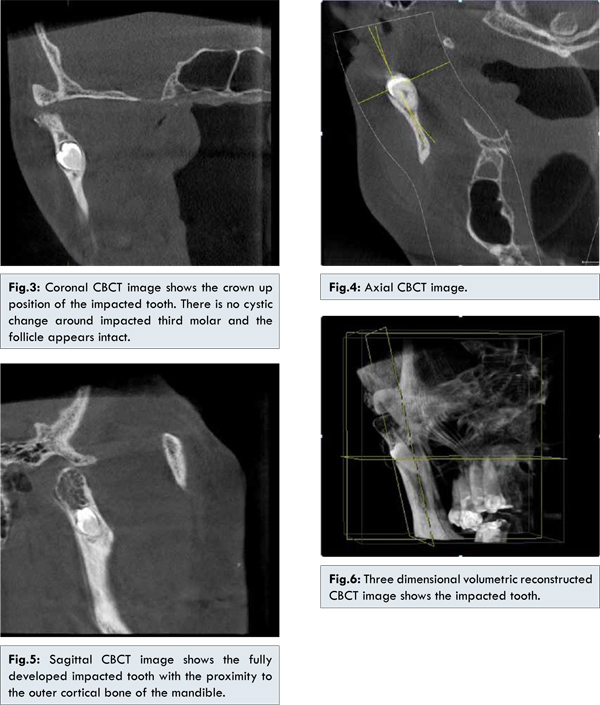
According to the orientation and location of the impacted tooth, it was considered as an ectopic impaction of a mandibular third molar. Cone beam CT scans were performed to evaluate the position and direction of the impacted tooth in the mandibular condyle. Coronal image showed the crown up position of the impacted tooth [Fig.3]. There was no sign of cystic change around the impacted tooth, the follicle space around the teeth appeared normal. On the axial image, an impacted tooth was found in the posterior border of ramus with close proximity to the lingual cortical plate [Fig.4]. Sagittal image showed a well developed impacted tooth in the subcondylar region with normal follicular space [Fig.5]. On the 3D volumetric image, the crown of the impacted tooth was positioned towards the lateral surface of condyle [Fig.6]. There was no pathologic or morphologic change on the surrounding bone. Final diagnosis was an ectopic impaction of the mandibular third molar in the right mandibular subcondyle.
The true incidence and etiology of ectopic impaction of mandibular third molar remain unknown. Several theories have been suggested to explain the ectopic eruption, including aberrant eruption, trauma, and ectopic formation of the germs of the teeth [2]. It has been suggested that an aberrant eruption pattern occurred when the tooth has been displaced by a lesion, usually an odontogenic cyst [3]. Wang et al. in 2008 reported a similar case and reviewed the literatures from 1978 to 2003. They found 13 case reports of the ectopic third molars in the subcondylar area, including 1 case of a dry skull and 1 of a cadaveric mandible. The management for these conditions was described as no treatment or as surgical removal via extraoral or intraoral access. Salmerón et al. in 2008 reported 2 cases of third molars in the subcondylar area, which were associated with odontogenic cysts and treated through the extraoral approach, indicating that the treatment was primarily determined by the experience of the surgeon or physician. Wang
et al. reviewed that eight of the 11 cases included the description of a radiolucent image around the ectopic molar on the radiograph, including 5 with the diagnosis of a dentigerous cyst. These mandibular third molars might be displaced by the lesion. The expansion of a cyst might put pressure on the crown of a tooth and displace it in the opposite direction to the path of eruption. Several teeth had an upward whereas the others had a downward inclination or even an inverted crown position [3]. In this case, the abnormal position of the tooth germ might be the most likely causative factor because the impacted tooth was positioned in the mandibular subcondyle region with an upward crown position without any pathologic change which resulted in such unusual movement. Jin-Soo Kim in 2008 probably reported the only case of ectopic third molar in condyle without any associated pathological condition and presented the relationship of impacted mandibular third molar to the surrounding anatomic structures using cone beam computed tomography [4]. Fernand Iglesias-Martin et al. in 2012 reported a similar case of ectopic third molar in left condylar region in an inverted position with a radiolucent image around third molar crown and reviewed literature from 1980 to 2011, they found 14 well documented clinical cases from the literature with a new clinical case provided by the authors, representing a sample of 15 patients. They found a mean age at diagnosis of 48.6 years and a higher prevalence in women. In 14 patients, associated radiolucent lesions were diagnosed on radiographic studies and confirmed histopathologically as odontogenic cysts. Most of the reported cases were associated with radiolucent lesions in panoramic radiographs and also confirmed histopathologically as dentigerous cysts [5]. Therefore the theory involving odontogenic cysts in the pathogenesis of ectopic third molar seemed to be most relevant. However, this case is unique because there is no radiolucent lesion surrounding the teeth in OPG and CBCT image, so the theory of ectopic formation of tooth germ could be considered or mal-eruption of a tooth into an ectopic location may too be considered. Thus the chemical factors that aid in eruption will need to be looked upon with more expectancy, such that they shed more light into the complex procedure of tooth eruption. The surgical removal of an ectopic mandibular third molar with acute inflammation or cystic lesion is recommended to prevent further complications such as diffuse osteolysis, condylar process deformity, or bone absorption [6,7]. In this case, the impacted tooth was not removed because of the absence of the associated symptom or lesion unlike other reports and the patient’s age [2,4,8]. Patient has been advised to be kept under observation with review radiographs once in every three years.
Conclusion
Ectopic third molar in the sub condylar region is rare. This case is probably the second reported case of ectopic third molar in the sub condylar region without any pathology. An OPG together with clinical examination is usually sufficient for diagnosis of an ectopic third molar. However, CBCT scans are sometimes required to determine a more precise anatomical position and its relation to adjacent structures.
References
- Alling CC 3rd, Catone GA. Management of impacted teeth. J Oral Maxillofac Surg 1993; 51(1 Suppl 1):3-6.
- Salmerón JI, del Amo A, Plasencia J, Pujol R, Vila CN. Ectopic third molar in condylar region. Int J Oral Maxillofac Surg 2008;37:398-400.
- Wang CC, Kok SH, Hou LT, Yang PJ, Lee JJ, Cheng SJ, et al. Ectopic mandibular third molar in the ramus region: report of a case and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:155-161.
- Jin-soo Kim. Cone beam computed tomography findings of ectopic mandibular third molar in the mandibular condyle: report of a case. Imaging science in dentistry 2011;41:135-137.
- Fernando Iglesias-Martin, Pedro Infante-Cossio, Eusebio Torres-Carranza, Victoria-Eugenia PratsGolcze, Alberto Garcia-Perla-Garcia. Ectopic third molar in the mandibular condyle: A review of the literature. Med Oral Patol Oral Cir Bucal. 2012;17(6):e1013-1017.
- Medici A, Raho MT, Anghinoni M. Ectopic third molar in the condylar process: case report. Acta Biomed Ateneo Parmense 2001;72:115-118.
- Gadre KS, Waknis P. Intra oral removal of ectopic third molar in the mandibular condyle. Int J Oral Maxillofac Surg. 2010;39:294-296.
- Wassouf A, Eyrich G, Lebeda R, Grätz KW. Surgical removal of a dislocated lower third molar from the condyle region: case report. Schweiz Monatsschr Zahnmed. 2003;113:416-420.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Joy E T, Khan F, Mohammed SOPG and CBCT Finding’s of an Ectopic Third Molar in the Sub-condylar Region.JCR 2014;4:286-290 |
|
Joy E T, Khan F, Mohammed SOPG and CBCT Finding’s of an Ectopic Third Molar in the Sub-condylar Region.JCR [serial online] 2014[cited 2026 Jul 31];4:286-290. Available from: https://www.casereports.in/articles/4/2/OPG-and-CBCT-Findings-of-an-Ectopic-Third-Molar-in-the-Sub-condylar-Region.html |

|
|
|
|
|