Introduction
Acute onset of weakness has got a long list of differential diagnosis with neurovascular causes being the most important. Nonetheless other causes have to be always ruled out before going for expensive imaging modalities. Electrolyte disturbances like simple hypokalemia, is known to cause muscle weakness and its correction promptly reverses the paralysis. In the setting of thyrotoxicosis, periodic paralysis has been rarely observed. It is usually attributed to an abnormality in the Na+/K+ ATPase pump due to the effect of excess thyroid hormones which cause an intracellular shift of potassium leading to hypokalemia in the presence of normal total body potassium [1]. The commonest cause of hyperthyroidism in these patients is Grave’s disease but other causes have also been described. It is worthy to note that this disorder can also present with normal K+ levels when it is measured in between the attacks. Another rare form of this disorder called thyrotoxic normokalemic periodic paralysis, also has normal K+ levels [2]. Here we present a 21 year old male patient who presented with paraplegia as the only symptom who was diagnosed to be thyrotoxic and treated with antithyroid drugs with complete resolution of the paralysis.
Case Report
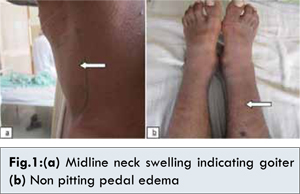
A 21 year old male patient presented with acute onset of complete weakness in both lower limbs. This was no history of similar complaints in the past. There was no familial history of similar attacks. On examination the patient had a central swelling of the neck with nonpitting bilateral pedal edema upto knee [Fig.1]. Fundus examination was normal. Nervous system examination revealed hypotonia in both lower limbs with grade 1/5 weakness and normal upper limbs. Reflexes could not be elicited and planter reflex was nonresponsive. Sensory system was intact with no involuntary movements. Other systems were normal.
Routine hemogram, urine analysis, blood sugar, blood urea, serum creatinine, creatine phosphokinase (CPK), serum Na+, K+ [Na+: 135 mEq/L, K+: 3.4 mEq/L] were within normal limits. Thyroid function test showed very low TSH levels (0.12 µIU/mL) with elevated T3 (3.4 ng/mL) and T4 (20.2 ng/mL) confirming a diagnosis of hyperthyroidism. A diagnosis of thyrotoxic periodic paralysis was made. K+ levels were normal even after repeated testing, during the paralysis and after the recovery.
The patient was started on antithyroid drug methimazole and propranolol. He recovered from the paraplegia within a day of starting the treatment; it took around 3 months to become euthyroid. He has remained asymptomatic till date on antithyroid drugs.
Discussion
Thyrotoxic periodic paralysis (TPP) is a potentially lethal neuromuscular complication of thyrotoxicosis seen in a very small percentage of patients. The patient can present with paraparesis or complete paralysis of limbs, axial muscle groups, dysarthria or ophthalmoplegia. Carl Friedrich Otto Westphal first described periodic paralysis [3]. The first case of thyrotoxic periodic paralysis was described by Rossenfield in 1902 [4]. It is seen in 13-24% of thyrotoxicosis cases in Asians, numerous cases have been reported from Japan and China. In this race it occurs 70 times more frequently in males than females and usually occurs between the ages of 20 and 40 years reflecting the age of onset of thyrotoxic Graves’ disease [1]. It is less commonly seen in Caucasians and Africans with very few cases reported from Indian subcontinent.
The exact pathogenesis in TPP is unknown but it likely involves defects in membrane bound ion-transporting proteins, such as sodium, K-adenosine triphosphatase [5], or ion channel proteins [6]. The mechanism of hypokalemia is explained by a sudden influx of potassium into muscle by increased activity of sodium potassium pumps. There is an increase in sodium-potassium ATPase activity in all patients who become thyrotoxic but in those individuals who are susceptible to periodic paralysis the increase in sodium-potassium ATPase activity is much higher despite similar degrees of hyperthyroidism [7]. Certain HLA antigen including A2, Bw22, Aw19, and DRW8 have been incrimated especially in males of Asian race [8].
The finding of a normal serum potassium level in this patient may be because he presented during the recovery phase of the paralysis. There have however been rare reports of normokalaemia during the paralytic phase of thyrotoxic periodic paralysis, the exact pathophysiology of which remains elusive.
Treatment consists of medical, surgical or radio-ablative therapy to maintain a euthyroid state. Antithyroid drugs and beta blockers can be used until patient reaches euthyroid state. Potassium supplementation is controversial as the total potassium levels are usually normal. It should be reserved only for cases with hypokalemia induced arrhythmias. Potassium sparing diuretics can also be used. Hyperthyroidism is usually subtle in these cases leading to delay in diagnosis and treatment [9].
TPP should be taken into consideration in the differential diagnosis of all acute episodes of motor paralysis especially in young patients. Judicious replacement of potassium and achievement of a euthyroid state is the mainstay of treatment. Accurate diagnosis is important as the condition is often mistaken for Gullian Barre especially when it presents with respiratory muscle paralysis leading to mistaken management and loss of precious time.
References
- Ahlawat SK, Sachdev A. Hypokalaemic paralysis. Postgrad Med J 1999;75:193-197.
- Wu CC, Chau T, Chang CJ, Lin SH. An unrecognized cause of paralysis in ED: thyrotoxic normokalemic periodic paralysis. Am J Emerg Med. 2003;21(1):71-73
- Westphal CF. A strange case of periodic paralysis of all four extremities with simultaneous extinction of electrical excitability during the paralysis. Berl. Klin. Wochenschr. (in German).1885;22:489-91 and 509-511.
- Rossenfield M. Acute ascending paralysis in Graves’ disease. Berl Klin Wochnschr 1902;39:538.
- Miller C. Potassium selectivity in proteins: oxygen cage or Pi in the face? Science 1993;261:1692-1693.
- Ackerman MJ, Clapham DE. Ion channels: basic science and clinical disease. N Engl J Med 1997;336:1575-1586.
- Chan A, Shinde R, Chow CC, Cockram CS, Swaminathan R. In vivo and in vitro sodium pump activity in subjects with thyrotoxic periodic paralysis. BMJ 1991;303:1096-1099.
- Tamai H, Tanaka K, Komaki G, Matshubayash S, Hirota Y, Mori K, et al. HLA and thyrotoxic periodic paralysis in Japanese patients. J Clin Endocrinol Metab 1987;64:1085.
- Kung AW. Clinical review. Thyrotoxic periodic paralysis: A diagnostic challenge. J Clin Endocrinol Metab 2006;91:2490-2495.