|
|
|
|
|
Successful Outcome of Pregnancy in Borderline Malignant Ovarian Tumor
|
|
|
Rajshree Dayanand Katke
From the Department of Obstetrics & Gynaecology, Grant Government Medical College & Sir J. J. Group of Hospitals, Mumbai, Maharashtra, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Rajshree D. Katke
Email: drrajshrikatke@gmail.com
|
|
|
|
|
|
|
|
|
Received:
15-AUG-2014 |
Accepted:
09-SEP-2014 |
Published Online:
15-OCT-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
We report a case of a 26 year-old young pregnant woman diagnosed as pregnancy with ovarian tumor having solid component within it. Laparotomy was done with removal of right ovarian tumor. Frozen sections revealed serous (cystic) tumor with borderline malignant potential. Her left ovary was preserved for fertility function. Patient withstood surgery well; induction of ovulation was done after 6 months and patient conceived. The whole course of pregnancy was uneventful except once when she had threatened preterm activity treated and pregnancy continued till term. Patient went in spontaneous labour and delivered normally with a healthy male baby. Her CA-125 on one year follow up was within normal limits. |
|
|
|
|
|
Keywords :
|
CA-125 Antigen, Ovarian Neoplasms, Pregnancy, Ovulation, Frozen Sections, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff50f8050000003703000001000900 6go6ckt5b5idvals|377 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Conservative and functional surgeries are increasingly being used in surgical oncology, with an aim to preserve the organ function. The evolution of new surgical procedures to reduce radical resection in oncological gynaecological surgery is a perfect example. Although radical surgery remains the `gold standard’ in the treatment of ovarian cancers, a conservative approach can be considered in patients with early-stage disease and in a young patients, in order to preserve their fertility function.
Around 2-3% of masses removed during pregnancy are found to be malignant and this is a key issue to be considered when counselling the patient [1,2]. Despite this fact, the great majority of high suspicion adnexal masses excised during pregnancy are in fact borderline ovarian tumors. Ovarian tumors of low malignant potential comprise 10-20% of all ovarian malignancies [3,4]. They carry an excellent prognosis with 95-99% long-term survival [3]
Case Report
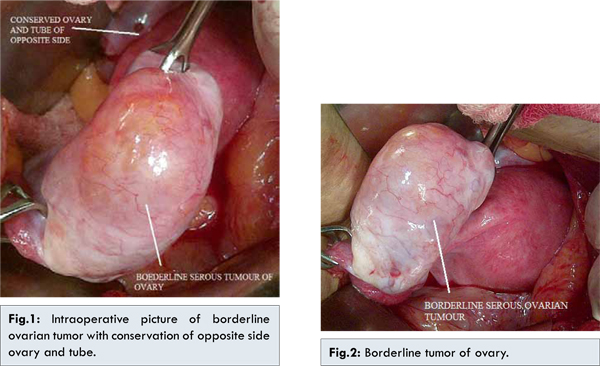
26-year-old young girl, married since two years was referred to us for abdominal pain and irregular menses (4-5 days /15-40 with moderate blood flow) since one year. Her past medical history was insignificant except she underwent medical termination of pregnancy at 10 weeks in view of CT scan radiation exposure. On general examination, she was afebrile, with a blood pressure of 120/78 mmHg and a pulse of 74 beats/min. Her per-abdominal examination revealed fullness in the right lower abdomen, 12x10x10 cm firm to cystic ill-defined mass, with restricted mobility. Per-speculum examination was normal. Per-vaginal examination revealed normal cervix and vagina with anteverted, anteflexed and normal size uterus. The above described mass could be felt through the right fornix. Left fornix was normal and rectal mucosa was free. The patient’s hematologic and biological workups were within normal limits except hypoproteinemia. Ultrasound investigation revealed a cystic mass measuring 7x6x6 cm in right ovary. This cystic formation had multiple thick nodular areas at periphery with a possibility of neoplastic etiology. Doppler study revealed anechoic cystic lesion measuring 8x7 cm with mural nodules and irregularity in right adnexa. No evidence of calcification/internal septations/echoes was seen. Minimal vascularity was seen in mural thickening, right ovary not visualized separately with features suggestive of complex right ovarian cyst. CT scan whole abdomen confirmed the ultrasound findings. Her CEA was within normal limits but CA-125 was raised above normal (1040.5 U/mL). Staging laparotomy revealed right ovarian tumor with normal left ovary on gross examination (FIGO stage Ia). Frozen section of right ovary revealed serous (cystic) tumor: borderline malignant potential. The decision regarding preservation of fertility was taken hence she underwent unilateral removal of tumor with ovary. Peritoneal washing cytology, sampling biopsies from the staging surgery were negative. Slides and paraffin blocks were reviewed at Tata hospital which was reported as serous (cystic) tumor: borderline malignant potential. Patient tolerated surgery well and post-operative period was uneventful. Patient was asymptomatic and was on regular follow up for 2 years. She was evaluated for infertility. Follicular study revealed lack of progressive development of follicles. Ovulation was induced with tablet clomiphene citrate 50 mg once daily for five days from second day of menses and follicular growth was monitored with the follicular study from 9th day of menses for 2 cycles and planned relationship was advised. She conceived after induction of ovulation. During her antenatal period she was admitted twice for threatened preterm labour which was managed conservatively with tocolysis and bed rest. Patient delivered full term healthy 2.7 kg male child. Postpartum period was uneventful and patient discharged on 4th day with healthy baby after vaccination. Her CA-125 tumor marker value was within normal limits postoperatively and on follow up at one year.
Borderline ovarian tumors (BOT) are a distinct histological entity and account for nearly 10-20% of all ovarian epithelial tumours [3-5]. Majority of borderline ovarian tumors are diagnosed in women of childbearing age (<40 years); however little is known about the epidemiology and management of these tumors diagnosed during pregnancy. According to the literature, borderline ovarian tumors are frequently diagnosed during the first trimester incidentally in routine ultrasound exams. When symptomatic, patients may refer to unspecific abdominal pain [3,6]. Pelvic ultrasound remains the mainstay for evaluating the adnexa.
Surgical staging is important issue in the management of borderline ovarian tumors [7-9]. Laparoscopic restaging surgery reduces the risk of postoperative adhesions and mechanically induced infertility. However, the harmless nature of this surgery in patients with ovarian cancer remains the subject of debate, and restaging surgery using midline laparotomy remains the current the `gold standard’. Conservative treatment provides good results for fertility, and does not affect the survival of patients with borderline ovarian tumour. This approach should be considered for young women desiring fertility, even if peritoneal implants are discovered at the time of the initial surgery. In case of infertility, the use of assisted reproduction techniques may be suggested to patients with stage I borderline ovarian tumor, with a limited number of stimulation cycles. In patients with epithelial ovarian cancer, conservative surgery of an ovary and the uterus can only be considered in adequately stratified patients with serous, mucinous or endometrioid tumor, excellent prognostic factors (stage IA, grade 1 or perhaps 2) and a careful follow-up. Removal of the ovary should be carried out when childbearing is complete.
In our case fertility sparing surgery was carried out in view of patient being young lady with borderline ovarian tumor and no living issue. The patient withstood surgery well and her tumor markers returned to normal during follow-up. Patient conceived after induction of ovulation. Her antenatal period was monitored closely and she successfully delivered a healthy 2.7 kg baby.
Conclusion
Borderline ovarian tumors represent a rare clinical entity. Each case needs individualized management based on the risk benefit ratio. While in women with a complete family- total abdominal hysterectomy with bilateral salphingo-oophorectomy is recommended, young women should undergo fertility sparing surgeries with close follow-up.
References
- Creasman WT, Fetter BF, Hammond CB, Parker RT. Germ cell malignancies of the ovary. Obstet Gynecol. 1979;53:226-230.
- Hart WR, Norris HJ. Borderline and malignant mucinous tumors of the ovary. Cancer. 1973;31:1031-1044.
- Bell DA, Weinstock MA, Scully RE. Peritoneal implants of ovarian serous borderline tumors. Histologic features and prognosis. Cancer. 1988;62:2212-2222.
- Gotlieb W, Flikker S, Davidson B, Korach, Y, Kopolovic J, Ben-Baruch G. Borderline tumors of the ovary: fertility treatment, conservative management and pregnancy outcome. Cancer. 1988;82:141-146.
- Morris RT, Gershenson DM, Silvia EG, Follen M, Morris M, Wharton JT. Outcome and reproductive function after conservative surgery for borderline ovarian tumors. Obstet Gynecol. 2000;95:541-547.
- Morice P, Camatte S, El Hassan J, Lhomme ÂC, Duvillard P, Castaigne D. Clinical outcomes and fertility results after conservative treatment for ovarian borderline tumor. Fertil Steril. 2001;75:92-96.
- Nijman HW, Burger CW, Baak JP, Schats R, Vermorken JB, Kenemans P. Borderline malignancy of the ovary and controlled hyperstimulation, a report of 2 cases. Eur J Cancer. 1992;28A:1971-1972.
- Zanetta G, Chiari S, Rota S, Bratina G, Maneo A, Torri V, Mangioni C. Conservative surgery for stage I ovarian carcinoma in women of childbearing age. Br J Obstet Gynaecol. 1997;104:1030-1035.
- Katke RD, Gadekar S, Pagare P. A rare case of carcinoma of ovary with carcinoma of cervix. Journal of Case Reports. 2014;4(1):217-220.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Katke RDSuccessful Outcome of Pregnancy in Borderline Malignant Ovarian Tumor.JCR 2014;4:391-394 |
|
Katke RDSuccessful Outcome of Pregnancy in Borderline Malignant Ovarian Tumor.JCR [serial online] 2014[cited 2026 Jun 21];4:391-394. Available from: https://www.casereports.in/articles/4/2/Successful-Outcome-of-Pregnancy-in-Borderline-Malignant-Ovarian-Tumor.html |

|
|
|
|
|