|
|
|
|
|
Successful Outcome of Triplet Pregnancy with Peripartum Cardiomyopathy
|
|
|
Rajshree Dayanand Katke, Ashish Zarariya
From the Department of Obstetrics & Gynaecology, Grant Government Medical College & Sir J. J. Group of Hospitals, Mumbai, Maharashtra, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Rajshree D. Katke
Email: drrajshrikatke@gmail.com
|
|
|
|
|
|
|
|
|
Received:
29-MAY-2014 |
Accepted:
11-SEP-2014 |
Published Online:
30-OCT-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Peripartum cardiomyopathy (PPCM) is a subset of dilated cardiomyopathy and its diagnosis is often delayed as it’s clinical features are considered physiological during pregnancy and postpartum period leading to lethal consequences. Triplet pregnancy itself is high risk for the mother due to greater hemodynamic perturbations, greater hormonal changes and greater demand on nutritional reserves, all of which could be involved in the pathophysiology of PPCM. We hereby report an interesting case of peripartum cardiomyopathy in triplet pregnancy with successful outcome. |
|
|
|
|
|
Keywords :
|
Triplet pregnancy, Pregnancy, Dilated cardiomyopathy, Postpartum Period, Peripartum Period, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff0400060000003f03000001000100 6go6ckt5b5idvals|383 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Peripartum cardiomyopathy is defined as onset of heart failure in the last month of pregnancy and first 5 months post-partum with no other etiology of heart failure identified and no history of cardiac disease. The dysfunction is characterised by a reduced ejection fraction. High risk factors include black race, advanced maternal age, multiparity, multiple gestation, pre-eclampsia and stress [1,2]. Symptoms include fatigue, edema, dyspnea which may lead to false diagnosis of other pregnancy co-morbidities such as pulmonary embolism and eclampsia [3]. The following case report illustrates a typical presentation of peripartum cardiomyopathy in a patient with triplet pregnancy with complete recovery after treatment.
Case Report
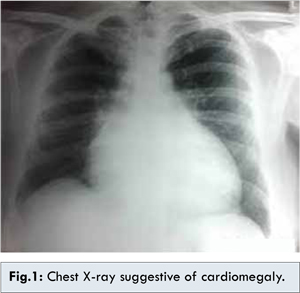
A 30 year old primigravida, married since 10 years, infertility conception, booked case at private hospital, 32 weeks by dates and by scan, with triplet gestation was admitted for safe confinement at our institute. Patient was mildly anaemic with no other risk factors. She was treated with oral hematinics and steroids. Routine ultrasound doppler study at 34 weeks was suggestive of first fetus in breech presentation with feto-placental insufficiency. Planned caesarean section was performed at 34 weeks under spinal anaesthesia. There were no intra or immediate post-partum complication to mother and fetus. Baby weights were 1.6 kg, 1.7 kg and 1.7 kg. One unit blood transfusion was given post-operatively in view of pre-operative haemoglobin 8.2 gm/dL. Sixteen hours after operation, patient complained of breathlessness and cough. Examination revealed bilateral crepitations on auscultation. Oxygen saturation was 84%. On further investigation chest X ray revealed cardiomegaly [Fig.1]. Electrocardiogram was within normal limits and echocardiogram revealed cardiomegaly with LVEF of 35% with grade 1 mitral regurgitation. Patient was treated with oxygen by nasal prongs, injection furosemide, tablet enalapril 2.5 mg, tablet carvedelol 3.125 mg and tablet aldactone 50 mg. On post operative day 5 patient was stable and maintaining saturation of 98% without oxygen. Patient was discharged on 24th postoperative day in healthy condition with healthy babies with a advice for barrier contraception and follow up 2-D Echo after 3-6 months.
Peripartum cardiomyopathy is often missed because dyspnea in a common finding during pregnancy and post-partum period and is the earliest symptom of peripartum cardiomyopathy. If pregnant women gain excessive amounts of weight, have significant lower-extremity edema, or have jugular venous distension in the presence of gallop rhythms or cardiomegaly then they should be referred for an echocardiogram. Normal pregnancy is associated with an increased heart rate and left ventricular diastolic function; there should not, however, be elevations in diastolic dimensions beyond normal levels or reductions in ventricular function during gestation or the postpartum period.
Women with suspected peripartum cardiomyopathy must undergo a careful medical and family history assessment and investigations to exclude pre-existing heart disease or intercurrent causes of left ventricular compromise. Chest radiography can reveal cardiomegaly, pulmonary congestion and sometimes pleural effusion [4]. Electrocardiogram findings are often normal hence an echocardiogram should be done to document ventricular size. In our case, the chest X-ray revealed cardiomegaly, electrocardiogram findings were normal but echocardiogram revealed cardiomegaly with LVEF of 35%. Treatment includes fluid restriction, use of diuretics, beta blockers and digoxin. Such patients are at high risk for thrombus formation [5]. Thus anticoagulation should be considered in patients with severe LV dysfunction. Irrespective of recovery further pregnancy should be avoided since it recurs in 30% of pregnancies [6]. Thus it is important to consider peripartum cardiomyopathy, when diagnosing dyspneic patients for faster initiation of treatment for a potentially lethal condition. Following discharge patients are seen at 2-week intervals. The echocardiogram should be repeated at these visits until ventricular function improves [7]. Once stable, the outpatient visit and echocardiogram interval is determined by the patient’s clinical state. With proper medication, diet and exercise, ventricular remodelling is usually complete within 6 months of initial presentation.
Conclusion
Diagnosing peripartum cardiomyopathy is a challenge to the physicians. Our case is a unique example where two high risk conditions of triplet pregnancy and peripartum cardiomyopathy were managed with successful outcomes by multidisciplinary approach in obstetric setup. Prompt diagnosis and treatment of peripartum cardiomyopathy had helped the mother to fight this lethal condition.
References
- Libby P, Bonow RO, Mann DL, Zipes DP. Braunwald’s heart disease: a textbook of cardiovascular medicine, 8th ed. Philadelphia: Saunders; 2007.
- Marx JA, Hockberger RS, Walls RM. Rosen’s emergency medicine: concepts and clinical practice, 6th ed. Philadelphia: Elsevier Health Sciences; 2006.
- Abboud J, Murad Y, Chen-Scarabelli C, Saravolatz L, Scarabelli TM. Peripartum cardiomyopathy: a comprehensive review. Int J Cardiol. 2007;118(3):295-303.
- Bhakta P, Biswas B, Banerjee B. Peripartum cardiomyopathy: review of the literature. Yonsei Med J. 2007;48(5):731-747.
- Walsh JJ, Burch GE, Black WC, Ferrans VJ, Hibbs RG. Idiopathic myocardiopathy of the puerperium (postpartal heart disease). Circulation. 1965;32:19-31.
- Libby P, Bonow RO, Mann DL, Zipes DP. Braunwald’s heart disease: a textbook of cardiovascular medicine, 8th ed. Philadelphia: Saunders; 2007.
- Chakrabarti S, Pan K. Acromegaly Presenting as Congestive Cardiac Failure. Journal of Case Reports. 2014;4(1):221-224.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Katke RD, Zarariya ASuccessful Outcome of Triplet Pregnancy with Peripartum Cardiomyopathy.JCR 2014;4:416-418 |
|
Katke RD, Zarariya ASuccessful Outcome of Triplet Pregnancy with Peripartum Cardiomyopathy.JCR [serial online] 2014[cited 2026 Aug 3];4:416-418. Available from: https://www.casereports.in/articles/4/2/Successful-Outcome-of-Triplet-Pregnancy-with-Peripartum-Cardiomyopathy.html |

|
|
|
|
|