Introduction
Many complications associated with cocaine use have been reported in the past. These include cocaine induced hypertensive emergencies, strokes, cocaine induced myocardial infarction (form coronary vasospasm) and infections such as HIV and infective endocarditis (associated with intravenous drug use). However, it is rare for a person to present with osteonecrosis of appendicular skeleton as a result of cocaine abuse.
The reason for writing this case report is to promote awareness. As physicians, we commonly see complications related to cocaine abuse (especially in the emergency department). In addition to the common presentations of cocaine abuse, we also come across rare presentations such as the one presented in this case. It is important for us to understand the underlying pathophysiology to help manage this specific patient population better. Complaints of pain from an individual with a history of drug abuse are usually not given much importance and labeled as “narcotic seeking behaviour” by many physicians across the world. However, some of these patients actually have “genuine pain”.
As physicians, we should be unbiased while managing such patients to prevent under treatment. Studies have shown that adequate management of co-existing medical conditions in such patients is associated with better outcomes and higher rates of quitting.
Case Report
48 year old with past medical history of hypertension, chronic obstructive pulmonary disease (COPD) and cocaine abuse presented to the emergency department because of sudden onset difficulty in breathing and cough. According to the patient, the cough and shortness of breath started 24 hours before the presentation, was sudden in onset and has got progressively worse. Cough was productive in nature with some brown colored sputum. He had no associated chest pain, fever or chills. He didn’t report any leg swelling or any history of travel. According to the patient, his last cocaine use was “15 years ago” but his urine toxicology report was positive for cocaine and amphetamines. Past records also revealed that the patient had been admitted to the hospital multiple times in the past for similar presentations secondary to cocaine abuse.
His review of systems was positive for chronic right knee pain (in addition to the symptoms described above). The patient informed us that he chronically takes NSAIDs for his knee pain. There was no history of any trauma to the knee in the past. Patient had no known drug allergies. His only medications were nifedipine for hypertension, inhaled tiotropium bromide for his COPD and naproxen for knee pain. Family history was only significant for hypertension in father. Social history was positive for homelessness for the past 3 month and patient reported living in a shelter for the same duration. Patient reported smoking half pack of cigarettes per day but denied any illicit
drug use.
Physical examination showed a poorly nourished individual, sitting on the bed, gasping for air and coughing. His blood pressure in the emergency department was found to be 185/97 mm Hg and heart rate was 106/min. Respiratory rate was 24/min. Auscultation of the chest revealed decrease breath sounds bilaterally as well as scattered wheezes in both lung fields. Examination of the right knee showed tenderness on deep palpation, but range of movement was normal. There was no redness or temperature change in the knee joint.
Patient had normal S1 and S2 without any murmurs or rubs. There was no jugular venous distension or pitting edema. Neurological examination showed that the patient was alert and oriented to time, place and person. He had normal sensation and 5/5 power in both upper and lower extremities. Coordination was also normal. Cranial nerve examination was also normal. Patient had down-going plantars on both sides and rest of the reflexes were also normal. Abdominal examination was also normal without any organomegaly. Patient had normal bowel sounds.
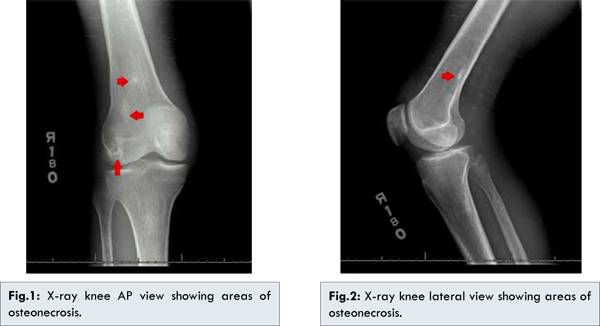
CBC with differential was normal (with hemoglobin of 11.8). Basic metabolic panel showed a creatinine of 1.40. Urine toxicology showed positivity for cocaine and amphetamines. Chest X-ray showed emphysematous change in both upper lung fields without any acute process. Knee X-ray was positive for multiple bone infarcts in the distal femur and proximal fibula. There were no joint abnormalities [Fig. 1,2].
Patient was admitted to the hospital for management of COPD exacerbation. Patient was started on prednisone 40 mg daily, albuterol and ipratropium nebulization every 4 hours. He was also started on doxycycline (due to change in sputum color). Acetaminophen was used as needed for pain. Within 2 days of admission, patient’s condition improved significantly. His breathing became less laboured and the wheezes in his chest disappeared. His nebulization treatments were switched to ‘as needed’ and the patient’s hemoglobin saturation remained about 92% on room air. Patient’s knee pain was also well managed on tylenol.
The primary team had a detailed discussion about the hazards of cocaine abuse with the patient. We also explained that the knee pain is also secondary to cocaine abuse as patient didn’t have any other risk factors for osteonecrosis (such as long term systemic steroids, sickle cell disease etc). The patient was advised to stop using cocaine and amphetamines and was provided with appropriate resources to help him quit. The patient was also advised to use acetaminophen instead of NSAIDs for knee pain to prevent complications such as gastritis and peptic ulcer.
The patient was discharged in a very stable condition and a follow-up appointment was scheduled with his primary care physician within the next 7 days.
Discussion
Cocaine is a crystalline alkaloid obtained from the leaves of the coca plant. Its characteristics include stimulation of CNS, appetite suppression and anesthesia at low doses. From a biological standpoint, it inhibits uptake of serotonin, norepinephrine and dopamine. It is addictive because of its effect on the mesolimbic reward pathway. Its effects on cardiac tissue are mainly due to sodium channels and therefore it has been linked to sudden cardiac deaths, mainly in drug abusers. It can easily cause the blood-brain barrier and can even disrupt it because of its molecular structure. It is controlled internationally by Single Convention on Narcotic drugs (Schedule I, preparation in Schedule III).
As physicians, it is fairly common for us to come across patients with history of cocaine (and multi-drug) abuse. Complications arising from cocaine abuse include hypertensive emergencies, strokes, acute kidney injury, cocaine induced bronchospasm, vasculitis etc. There have been many reported cases of “cocaine-levamisole syndrome” presenting with skin and other soft tissue necrosis [
1].
In previously reported cases, cocaine induced sinonasal osteocartilaginous necrosis has been reported (after snorting cocaine, resulting in severe vasoconstriction in the nasal mucosa) [
2-
5]. However, to our knowledge, cocaine induced necrosis of larger bones such as femur and fibula has not been reported. Purpose of presenting this case report is to create awareness among physicians about the hazardous effects of cocaine. Secondly, appropriate work-up should be done for an individual before labeling them as “narcotic seeking”. Understanding the pathophysiology of their underlying condition is crucial for their management.
Conclusion
It is important to recognize complications of acute and chronic cocaine use. In patients with history of drug use, narcotics-seeking behaviour is fairly common. However, the possibility of “real pain” should always be kept in mind and appropriate investigations should be ordered based on degree of clinical suspicion. Management of co-existing medical condition in such patient population can lead to better outcomes and higher rates of quitting.
References
- Ching JA, Smith DJ Jr. Levamisole-induced necrosis of skin, soft tissue, and bone: case report and review of literature. J Burn Care Res. 2012;33(1):e1-5.
- Ziraldo L, O’Connor MB, Blake SP, Phelan MJ. Osteonecrosis following alcohol, cocaine, and steroid use. Subst Abus. 2011;32(3):170-173.
- Trimarchi M, Nicolai P, Lombardi D, Facchetti F, Morassi ML, Maroldi R, et al. Sinonasal osteocartilaginous necrosis in cocaine abusers: experience in 25 patients. Am J Rhinol. 2003;17(1):33-43.
- Seyer BA, Grist W, Muller S. Aggressive destructive midfacial lesion from cocaine abuse. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(4):465-470.
- Kuriloff DB, Kimmelman CP. Osteocartilaginous necrosis of the sinonasal tract following cocaine abuse. Laryngoscope. 1989;99(9):918-924.