|
|
|
|
|
Cardiovocal or Ortner’s Syndrome due to Aortic Arch Pseudoaneurysm
|
|
|
Manjit Bagul1, Rajesh Mehra1, Priynath Agrawal2
1Consultant Radiologist, Venus Diagnostic Centre, Bhopal; 2Consultant Pulmonologist, Agrawal Hospital, Bhopal, Madhya Pradesh, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Manjit Bagul
Email: manjitbagul84@gmail.com
|
|
|
|
|
|
|
|
|
Received:
23-AUG-2016 |
Accepted:
30-AUG-2016 |
Published Online:
05-SEP-2016 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Cardiovocal or Ortner’s syndrome is unilateral vocal cord (VC) palsy due to non-malignant intrathoracic or cardio-vascular abnormality causing compression of recurrent laryngeal nerve (RLN) in the mediastinum. Left RLN palsy is more common due to longer mediastinal course along the aortic arch. We describe a case of a 60-year-old male patient complaining of hoarseness of voice. Laryngoscopy showed left vocal cord palsy without obvious laryngeal mass. CECT study of the neck and chest revealed aortic arch pseudo-aneurysm with left vocal cord palsy. The diagnosis of cardiovocal syndrome was confirmed. It is important for the radiologist to be aware of cardiovascular related hoarseness and CECT neck and chest should be included during the evaluation of VC palsy. |
|
|
|
|
|
Keywords :
|
Aneurysm, Aorta, Hoarseness, Laryngoscopy, Recurrent Laryngeal Nerve, Vocal Cord Paralysis.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffe819100000000205000001000300 6go6ckt5b5idvals|658 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Hoarseness of voice due to left recurrent laryngeal nerve paralysis was first described in 1897 by Norbert Ortner, an Austrian physician, in a patient with mitral valve disease (mitral stenosis and left atrial enlargement) [1-3]. Since then various cardiopulmonary conditions associated with left recurrent laryngeal nerve palsy, have been described, over the last 100 years. Thus, the syndrome is now also termed as cardiovocal syndrome. Here we present a case report of Ortner’s syndrome due to aortic arch pseudoaneurysm causing left recurrent laryngeal nerve palsy and discuss its CECT features in 60 year old male patient.
Case Report
A 60-year-old patient presented with the history of hoarseness of voice and dry cough since few weeks. Patient was known hypertensive and bidi smoker since many years. No past history of major illness was present. No other significant neurological or cardiorespiratory symptoms were found. Clinical examination was normal with no lump or mass in the neck region. Chest radiograph demonstrated mild emphysematous changes in the both lungs with unfolding of aorta. Atherosclerotic changes were noted in the arch of aorta with wall calcification of chest radiograph. No abnormal mass in the lungs or mediastinum was demonstrated on chest radiograph. Laboratory examination including complete blood count showed no remarkable abnormality.
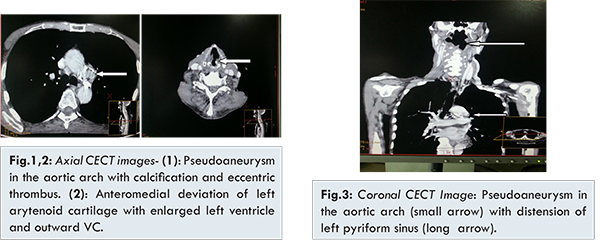
Laryngoscopy revealed left vocal cord palsy without any mass lesion in the larynx and paramedian position of the left vocal cord. Right vocal cord showed normal position. Patient further underwent CECT neck and chest to evaluate for the possible neoplastic etiology in neck or chest. The CECT examination [Fig.1-3] revealed left vocal cord palsy with antero-medial deviation of ipsilateral arytenoid cartilage and cricoarytenoid junction. Left pyriform fossa (PFS) showed significant distension normal appearing right PFS and right vocal cord position. No mass lesion was seen in vocal cords, larynx or neck spaces. Chest CT showed small pseudoaneurysm of aortic arch with calcific atherosclerotic plaques and small eccentric thrombus. No abnormal mediastinal or lung mass was seen. Mild emphysematous changes were noted in the both lungs with few healed calcified granulomas. The clinical symptoms in combination with laryngosscopy and imaging findings were consistent to that of cardiovocal or Ortner’s syndrome. Pseudoaneurysm of aortic arch was responsible for stretching of the left recurrent laryngeal nerve and resultant left vocal cord palsy.
The RLNs are the branches of vagus nerves providing the motor innervation to the intrinsic laryngeal muscles for vocalization exhibiting different course on right and left side. On the right side, the vagus nerve descends with the carotid artery sheath into the upper mediastinum. The right RLN exits from the vagus nerve anterior to the subclavian artery and courses posteriorly under the artery at the level of the brachiocephalic bifurcation. It has a short mediastinal course, coursing obliquely toward the right trachea-esophageal groove over the surface of the apical parietal pleura [1]. The left recurrent laryngeal nerve is longer and it branches from the vagus nerve at the level of the transverse aortic arch. It hooks under the arch of aorta, posterior to the ligamentum arteriosum before ascending towards the neck between the trachea and the esophagus [1].
The right RLN is 5-6 cm in length whereas the left RLN is nearly 12 cm in length with much of its course being mediastinal. For this reason, the left RLN is more vulnerable to stretch or compression neuropathy from mediastinal abnormalities [2]. In 1897, Ortner described a series of 3 cases of mitral stenosis suffering from hoarseness of voice because of left recurrent laryngeal nerve palsy. He suggested the cause to be compression of the left recurrent laryngeal nerve by an enlarged left atrium [3]. The most common mediastinal causes of VCP include lung cancer, aortic dissection, metastatic disease, tuberculosis, and esophageal cancer [4]. Common cardiovascular disorders responsible for the vocal cord palsy include aortic dissection, pseudoaneurysm, left atrial enlargement, mitral stenosis, congenital heart diseases, pulmonary artery enlargement and pulmonary embolism [5,6]. Iatrogenic unilateral cord palsy usually occurred due to damage of anterior broncho-esophageal artery supplying the left and inferior thyroidal artery supplying the right recurrent laryngeal nerve [7]. Our patient was known hypertensive with atherosclerotic aortic disease. CT findings showed the left vocal cord palsy with pseudo-aneurysm in aortic arch and no abnormal mass lesion in the neck spaces or mediastinum. Aortic arch pseudo-aneurysm can lead to compression of the left recurrent laryngeal nerve in the vulnerable space along the aortic arch. Sudden development of hoarseness due to vocal-cord palsy in patients with aneurysm has been recognized as a possible predictor of rupture of the aneurysm, since it is a sign of possible enlargement of the aneurysm [5]. In our case no obvious signs of aneurysmal rupture were observed. Chest radiograph is the first imaging study to rule out possible mediastinal or lung mass as cause of vocal cord palsy. Neck and chest CT and/or MRI should be done for all patients with left recurrent nerve palsy, because of the many possible etiologies. The imaging should include the entire course of the left recurrent laryngeal nerve. In a larger study of patients with left recurrent laryngeal nerve palsy aorto-pulmonary area was normal in 72% of the cases on chest radiographs but CT demonstrated a mass lesion [8].
Radiologists must be aware of this syndrome and should be able to differentiate cardiovocal syndrome from other pulmonary or mediastinal masses and based on the findings suggest the etiology directing the treatment of the patient. Prognosis of this syndrome depends on the underlying cardiovascular condition and correction of the underlying cardiac or vascular anomaly is important to a successful recovery. In our patient conservative management and voice therapy was done.
Conclusion
Ortner’s or cardiovocal syndrome is a rare condition characterized by vocal cord palsy secondary to various cardiopulmonary disorders. Aortic pseudoaneurysm is important cardiovascular cause of vocal cord palsy and it is therefore necessary to evaluate neck and chest region of patient with voice hoarseness. CECT neck and chest is most imporatant imaging modality to identify this disorder and differentiate various cardiopulmonary disorders responsible for vocal cord palsy.
References
- Laine FJ, Underhill T. Imaging of the lower cranial nerves. Neuroimaging Clin N Am. 2004;14(4):595-609.
- Delorme S, Knopp MV, Kauczor HU. Recurrence paralysis: computed tomographic analysis of intrathoracic findings [in German]. Radiologe. 1992;32(9):430-435.
- Ortner N. Recurrent nerve palsy in patient with mitral stenosis (in German). Wien Klin Wochenschr. 1897;10:753-755.
- Bando H, Nishio T, Bamba H, Uno T, Hisa Y. Vocal fold paralysis as a sign of chest diseases: a 15- year retrospective study. World J Surg. 2006;30(3):293-298
- Paquette CM, Manos DC, Psooy BJ. Unilateral vocal cord paralysis: a review of CT findings, mediastinal causes, and the course of the recurrent laryngeal nerves. Radiographics. 2012;32:721-740.
- Mohamed AL1, Zain MM, Hoarseness of voice in a patient with mitral stenosis and Ortner’s syndrome. Malays J Med Sci. 2004;11(2):65-68.
- Filaire M1, Garçier JM, Harouna Y, Laurent S, Mom T, Naamee A, et al. Intrathoracic blood supply of the left vagus and recurrent laryngeal nerves. Surgical and Radiologic Anatomy. 2001;23(4):249-252.
- Glazer HS, Aronberg DJ, Lee JKT, Sagel SS. Extralaryngeal causes of vocal cord paralysis: CT evaluation. American Journal of Roentgenology. 1983;141(3):527-531.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Bagul M, Mehra R, Agrawal PCardiovocal or Ortner’s Syndrome due to Aortic Arch Pseudoaneurysm.JCR 2016;6:420-423 |
|
Bagul M, Mehra R, Agrawal PCardiovocal or Ortner’s Syndrome due to Aortic Arch Pseudoaneurysm.JCR [serial online] 2016[cited 2026 Jul 4];6:420-423. Available from: https://www.casereports.in/articles/6/3/Cardiovocal-or-Ortners-Syndrome-due-to-Aortic-Arch-Pseudoaneurysm.html |

|
|
|
|
|