6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff24fd190000001d06000001000100
6go6ckt5b5idvals|764
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Point of care ultrasonography (POCUS) is the current management of emergency patient for two decades in Emergency Department (ED). McConnell sign is a possible finding of acute cor-pulmonary disease identified in POCUS described as a motion of apex of dilated right ventricle directed inside in systole.
Case Report
A 76 year old man was referred to the ED with flank pain and urolithiasis. However, he had dyspnea. At his triage examination his temperature was 36°C, heart rate was 91 beats/min, respiratory rate was 23/min, blood pressure was 100/60 mm Hg, oxygen saturation was 82% in room air, and blood glucose was 138 mg/dL.
No murmurs, clicks, rubs, or gallops were detected upon cardiac auscultation. Pulmonary examination revealed bilateral rales with decreasing frequency, decreased respiratory sounds, and elongated expiration. There was no tenderness in the lower extremities, color and temperature were normal. The patient exhibited 1+ pretibial edema. The only additional significant finding of the physical examination was left costochondral angle tenderness. The patient excreted 450 cc of urine in the urinary catheter that had been placed in the emergency department (ED).
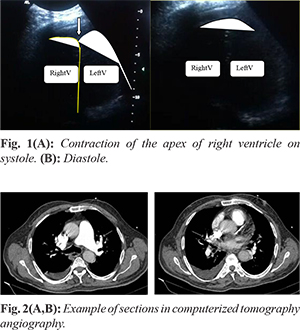
The electrocardiogram (ECG) revealed the presence of a right bundle block. Point-of-care cardiac ultrasound was performed in the ED to assist in the differential diagnosis of this critical patient. A large-curve transducer (Philips HDI 5000 C5-2R 15 Hz transducer), the only one could be reached was used to examine the apical four-chamber view on the patient in full sitting position and leaning forward. This was the only device at the point of care in ED at that moment. The patient was obese and could not tolerate a reclined position. Visual evaluation of the apical four chamber view using POCUS showed significant myocardial contractility of apex despite free wall hypokinesis of the dilated right ventricle (RV) with a hypertrophic and hyperkinetic left ventricle on video [Fig.1]. Computed tomography (CT) angiography of the chest demonstrated pulmonary thromboembolism of the bilateral branches of the pulmonary arteries [Fig.2] with frosted glass appearance, cardiomegaly, and pleural effusion of the right side. The physical examination and vital signs, diagnosis, clinical management and hospitalization decision occurred within approximately five minutes as a result of the use of POCUS.
Discussion
POCUS is a component of patient management in the ED that has been researched and developed since the 1990s. Focused cardiac ultrasound can be used to evaluate global function, pericardial effusion, and right ventricle dilatation [
1]. In addition, the McConnell sign with a dilated right ventricle is identified as pulmonary thromboembolism by POCUS.
The McConnell sign is a significant regional wall motion contractility of the apex though akinesis or hypokinesis of the middle and base of the free wall of the right ventricle in systole [
2,
3]. It is interpreted as the effect of increased effort of the left ventricle at its apex requiring compensation for the abnormal size, function and pressure of the right ventricle. McConnell reported RV dysfunction with akinesia of the RV mid-free wall by comparing quantitative and qualitative segmental motion during acute pulmonary embolism, pulmonary hypertension, and in normal control cases. This technique is reported to have 77% sensitivity and 94% specificity for the diagnosis of acute pulmonary embolism, with a positive predictive value of 71% and a negative predictive value of 96% [
4]. In another study, the McConnell sign had 96% specificity and 16% sensitivity when transthoracic echocardiography findings were analyzed within 48 hours of CT for pulmonary embolism [5]. There are several potential explanations for abnormal RV wall motion, including right ventricle infarct, and pulmonary hypertension [
6]. However, abnormal RV free wall motion in pulmonary hypertension is distinct in that it affect all regions of the tissue [
4]. Consequently, emergency medicine has to solve the acute clinical problems by providing the differential diagnosis and medical care in a short time. POCUS is the facilitator in this process. Even an old and large probe used for breast ultrasound prior in another clinic can solve the emergency question at point of care in a short time.
The McConnell sign with a dilated right ventricle on POCUS confirmed the bilateral thromboembolus on pulmonary branches. This was of significant help in the differential diagnosis, treatment, correct primary consultation, and hospitalization of this emergent and critical patient.
Contributors: BG: Manuscript writing, case management; EK: manuscript revision, radiological investigations; EK will act as guarantor. Both authors approved final version of the manuscript.
Funding: None; Competing interests: None stated.
References
- Via G, Hussain A, Wells M, Reardon R, ElBarbary M, Noble VE, et al. International evidence-based recommendations for focused cardiac ultrasound. J Am Soc Echocardiogr. 2014;27:683.e1-683.e33.
- Brenes-Salazar JA. McConnell’s echocardiographic sign in acute pulmonary embolism: still a useful pearl. Heart Lung Vessel. 2015;7:86-88.
- Haller EP, Nestler DM, Campbell RL, Bellamkonda VR. Point-of-care ultrasound findings of acute pulmonary embolism: McConnell sign in emergency medicine. J Emerg Med. 2014;47:19-21.
- McConnell MV, Solomon SD, Rayan ME, Come PC, Goldhaber SZ, Lee RT. Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism. Am J Cardiol. 1996;78:469-473.
- Lodato JA, Ward RP, Lang RM. Echocardiographic predictors of pulmonary embolism in patients referred for helical CT. Echocardiography. 2008;25:584-590.
- Platz E, Hassanein AH, Shah A, Goldhaber SZ, Solomon SD. Regional right ventricular strain pattern in patients with acute pulmonary embolism. Echocardiography. 2012;29: 464-470.