|
|
|
|
|
Shadow Cells Meet Keratin: A Rare Follicular Hybrid Cyst of Epidermal and Pilomatricoma Origin
|
|
|
|
Arushi Gupta1, Shaaan Khetrapal1, Zeeba. S. Jairajpuri1, Fahad2 Departments of 1Pathology and 2Surgery, Hamdard Institute of Medical Sciences and Research, Jamia Hamdard, New Delhi 110062, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr Shaan Khetrapal Email: shaankhetrapal@gmail.com |
|
|
|
|
|
|
|
|
Received:
27-MAY-2025 |
Accepted:
17-NOV-2025 |
Published Online:
25-MAY-2026 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: Follicular hybrid cysts (FHCs) are uncommon cutaneous lesions characterized by the co-existence of two or more distinct follicular components within a single cystic structure. Because of their nonspecific clinical appearance, they are frequently misdiagnosed as common benign cystic lesions. Histopathological examination plays a crucial role in establishing the correct diagnosis. Case Report: We report a case of a 68-year-old male who presented with a slow-growing nodular lesion over the back. The lesion was clinically suspected to be a benign cutaneous cyst. On histopathological examination, the cyst showed characteristic features of both epidermoid cyst and pilomatricoma, including keratinizing squamous epithelium and the presence of shadow cells. These findings confirmed the diagnosis of a follicular hybrid cyst composed of epidermoid and pilomatricoma components. Conclusion: Follicular hybrid cysts are rare lesions that may pose a diagnostic challenge due to their overlapping clinical features with other adnexal cysts. Recognition of their distinct histological components is essential for accurate diagnosis. Awareness of such unusual combinations helps clinicians and pathologists differentiate them from other cutaneous adnexal tumors and ensures appropriate management. |
|
|
|
|
|
Keywords :
|
Epidermal Cyst, Follicular Hybrid Cyst, Histopathology, Pilomatricoma, Skin Neoplasms.
|
|
|
|
|
|
|
|
|
|
|
|
Introduction
Follicular hybrid cysts (FHCs) are rare cutaneous lesions characterized by the co-existence of two or more distinct cystic components derived from different segments of the pilosebaceous unit. These lesions are uncommon and only sporadically reported in the literature. The term follicular hybrid cyst was first introduced by McGavran and Binnington in 1966 when they described a cystic lesion showing features of both epidermal and trichilemmal differentiation within the same structure. This observation highlighted the possibility of dual follicular differentiation occurring in a single lesion and generated interest among dermatopathologists [ 1]. Later, Requena and Sanchez expanded the concept of FHCs in 1991 to include cystic lesions demonstrating combinations of different follicular structures. These may include epidermoid (infundibular) cysts, trichilemmal cysts, pilomatricoma, eruptive vellus hair cysts, steatocystoma, and apocrine hidrocystoma. The common feature among these components is their origin from different parts of the hair follicle apparatus and associated adnexal structures [2]. The presence of two histologically distinct follicular lesions within a single cystic structure is uncommon and suggests a complex pattern of follicular differentiation, possibly arising from pluripotent stem cells located in the hair follicle bulge. Among the various combinations reported, the co-existence of epidermoid cyst and pilomatricoma is particularly rare. Therefore, we report this case of a follicular hybrid cyst composed of epidermoid cyst and pilomatricoma occurring on the back of a 68-year-old male to highlight its unusual histopathological features.
Case Report
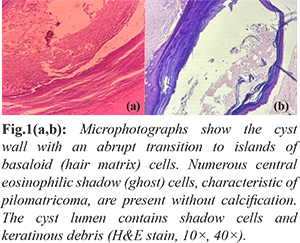
A 68-year-old male presented to the general surgery outpatient department with a complaint of a swelling over the mid-back region that had gradually increased in size over the past one year. The swelling was painless and was not associated with discharge, redness, or any systemic symptoms. There was no history of trauma, fever, or previous surgical procedures at the site. On clinical examination, a solitary swelling was noted in the midline of the upper back. The lesion appeared as a well-defined, dome-shaped nodule measuring approximately 1.5 cm in diameter. The overlying skin was unremarkable, and the swelling was non-tender and mobile on palpation. Based on the clinical findings, a provisional diagnosis of sebaceous cyst was made, and complete surgical excision was advised for both therapeutic and diagnostic evaluation. The excised specimen was submitted for histopathological examination. On gross examination, the specimen consisted of a globular, firm, grey-white to grey-brown tissue measuring 1.5×1×0.5 cm. The cut surface showed a well-circumscribed cystic cavity measuring approximately 1 cm in diameter, containing yellowish-white pultaceous material suggestive of keratinous debris. Microscopic examination of hematoxylin and eosin-stained sections revealed a dermal-based cystic lesion with mixed histological features. One portion of the cyst wall was lined by stratified squamous epithelium with a well-formed granular layer, consistent with an epidermoid (infundibular) cyst. The lumen of this component contained laminated keratin. Adjacent to this area, the cyst wall showed an abrupt transition to another component composed of nests and islands of basaloid cells resembling hair matrix cells. Within the central portions of these islands, numerous eosinophilic shadow (ghost) cells were identified, which are characteristic of pilomatricoma. Calcification was not observed in the sections examined. The lumen in this region contained a mixture of shadow cells and keratinous debris [Fig.1a,b].
The surrounding dermis exhibited a mild inflammatory infiltrate composed of lymphocytes, plasma cells, and occasional multinucleated giant cells, indicating a foreign body-type reaction. The adjacent adnexal structures were unremarkable [Fig.2]. A distinct transitional zone was identified where the squamous epithelial lining of the epidermoid cyst merged with the pilomatricoma component. Based on the combined histopathological features, a final diagnosis of follicular hybrid cyst composed of epidermoid cyst and pilomatricoma components was established.
Discussion
Epidermoid cysts are among the most common benign cystic lesions of the skin. They arise from the infundibular portion of the hair follicle and are lined by stratified squamous epithelium with a well-developed granular layer. The lumen of these cysts typically contains laminated keratinous material. In contrast, pilomatricoma, also referred to as calcifying epithelioma of Malherbe, is a benign adnexal tumor derived from hair matrix cells. Histologically, it is characterized by well-circumscribed dermal nodules composed of basaloid cells resembling immature hair matrix and shadow (ghost) cells, which represent anucleate keratinized cells with central pale areas indicating loss of nuclei. Follicular hybrid cysts represent a rare group of lesions that exhibit mixed histological features reflecting differentiation toward more than one component of the pilosebaceous unit. Various combinations have been described in the literature, including epidermoid cyst with trichilemmal cyst, trichilemmal cyst with pilomatricoma, eruptive vellus hair cyst with steatocystoma, and rarely, epidermoid cyst with apocrine hidrocystoma. The present case represents a rare hybrid lesion composed of epidermoid cyst and pilomatricoma components. Such combinations are uncommon, with only a limited number of cases reported in the literature. Takeda et al. reviewed 15 cases of follicular hybrid cysts in Japan, where the majority involved a combination of epidermoid and trichilemmal cysts and were predominantly located on the scalp and face [3]. Similarly, five cases of follicular hybrid cysts were reported in Korea, four of which demonstrated a combination of epidermoid cyst and pilomatricoma components, similar to the present case [4-7]. Several other studies have also documented hybrid lesions showing combined features of epidermoid cyst and pilomatricoma, indicating that although rare, the coexistence of these two follicular components within a single lesion is a recognized phenomenon [8-12]. The exact pathogenesis of follicular hybrid cysts remains uncertain, and several theories have been proposed. One hypothesis suggests that keratinous material from an epidermoid cyst may induce a foreign body granulomatous reaction, which subsequently triggers pilomatricoma-like differentiation. However, this explanation does not adequately account for the organized architecture and distinct morphological features of the pilomatricoma component observed in such lesions. Another theory proposed by Leppard and Bussey [13] and later supported by King [14] suggests that follicular hybrid cysts may represent a transitional stage in which one type of lesion evolves into another. Nevertheless, histological findings do not strongly support this concept, particularly because keratohyalin granules characteristic of epidermoid cysts are absent in pilomatricomas as well as in the transitional areas of hybrid cysts. Currently, the most widely accepted explanation is that these lesions originate from pluripotent or multipotential stem cells located in the bulge region of the hair follicle. These stem cells have the capacity to differentiate into multiple components of the pilosebaceous unit, thereby giving rise to cysts demonstrating more than one line of follicular differentiation. The presence of a clear transitional zone between the different components, as observed in the present case, further supports this theory. An additional observation reported in the literature is the occurrence of pilomatricoma-like changes within epidermoid cysts in patients with Gardner’s syndrome. Gardner’s syndrome is an autosomal dominant condition caused by mutations in the APC gene and is characterized by intestinal polyps, multiple epidermoid cysts, osteomas, and desmoid tumors. Cooper and Fechner described pilomatricoma-like changes in epidermoid cysts in a patient with Gardner’s syndrome, suggesting that genetic factors may contribute to the development of certain hybrid lesions [15]. Clinically, follicular hybrid cysts often resemble simple epidermoid or sebaceous cysts because of their benign appearance and slow growth. They are usually asymptomatic and commonly occur on the scalp, face, trunk, or extremities. Therefore, accurate diagnosis largely depends on histopathological examination, where identification of distinct morphological components within the same lesion is essential. Complete surgical excision is the treatment of choice for these lesions. Adequate removal generally results in an excellent prognosis, although incomplete excision may lead to recurrence. Despite their benign nature, recognition of follicular hybrid cysts is important for avoiding diagnostic confusion and for understanding the diverse differentiation potential of adnexal tumors.
Conclusion
The present case highlights an unusual hybrid cyst composed of an epidermoid cyst and pilomatricoma, confirmed on histopathological examination by the presence of two distinct epithelial components with a clear transitional zone. Recognition of this rare entity is important for accurate diagnosis and to avoid confusion with other adnexal tumors. Complete surgical excision is curative and associated with an excellent prognosis.
Contributors: AG: concepts, manuscript preparation & review; SK: design, definition of intellectual content, literature search, manuscript editing and review, guarantor; ZSJ: design, literature search, manuscript editing; FA: literature search, manuscript review. All authors approved the final version of this manuscript and are responsible for all aspects of this study. Funding: None; Competing interests: None stated.
References - MacGavran MH, Binnington B. Keratinous cysts of the skin. Identification and differentiation of pilar cysts from epidermal cysts. Arch Dermatol. 1966;94:499-508.
- Requena L, Sanchez YE. Follicular hybrid cysts. Am J Dermatopathol. 1991;13:228-233.
- Takeda H, Miura A, Katagata Y, Mitsuhashi Y, Kondo S. Hybrid cyst: case reports and review of 15 cases in Japan. J Eur Acad Dermatol Venerol. 2003;17:83-86.
- Lee MG, Lee WS, Chun SI. A case of epidermal cyst with pilomatricoma-like change. Korean J Dermatol. 1988;26:98-101.
- Cho SY, Whang KK, Hahm JH. Pilomatricoma combined with epidermoid cyst. Ann Dermatol. 2000;12:155-159.
- Jang HC, Park JS, Park G, Chung H, Kim SW. A case of a follicular hybrid cyst (epidermal cyst and pilomatricoma). Ann Dermatol. 2005;17:45-47.
- Woo SH, Yu DS, Song HJ, Oh CH. A case of a hybrid cyst composed of an epidermal cyst and a pilomatricoma. Korean J Dermatol. 2005;43:422-424.
- Pujani M, Agarwal S, Goyal RK, Jyotsna PL, Teiwani N, Rautela A. Pilomatricoma coexisting with epidermal cyst. Int J Dermatol. 2012;51:624-625.
- Tsuji N, Kurokawa I, Tomie K, Omoto Y, Senba Y, Habe K, et al. Epidermal cyst with pilomatoricoma (follicular hybrid cyst): immunohistochemical study with epithelial keratins and filaggrin. J Dermatol. 2010;37:922-925.
- Urabe K, Xia J, Masuda T, Moroi Y, Furue M, Matsumoto T. Pilomatricoma-like changes in the epidermal cysts of Gardner syndrome with an APC gene mutation. J Dermatol. 2004;31:255-257.
- Benharroch D, Sacks MI. Pilomatoricoma associated with epidermal cyst. J Cutan Pathol. 1989;16:40-43.
- Terada T. Cutaneous hybrid tumor composed of epidermal cyst and cystic pilomatricoma expressing p53 and high Ki-67 labeling. Int J Clin Exp Pathol. 2013;6(6):1187-1189.
- Leppard BJ, Bussey HJ. Gardner’s syndrome with epidermoid cysts showing features of pilomatrixomas. Clin Exp Dermatol. 1976;1:75-82.
- King LS. Mummified epidermal cysts (so-called "calcified epitheliomas"). Am J Pathol. 1947;23:29-41.
- Cooper PH, Fechner RE. Pilomatricoma change in the epidermal cysts of Gardner’s syndrome. J Am Acad Dermatol. 1983;8:639-644.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Gupta A, Khetrapal S, Jairajpuri Z S, FahadShadow Cells Meet Keratin: A Rare Follicular Hybrid Cyst of Epidermal and Pilomatricoma Origin.JCR 2026;16:42-45 |
|
Gupta A, Khetrapal S, Jairajpuri Z S, FahadShadow Cells Meet Keratin: A Rare Follicular Hybrid Cyst of Epidermal and Pilomatricoma Origin.JCR [serial online] 2026[cited 2026 Aug 1];16:42-45. Available from: https://www.casereports.in/articles/16/2/Shadow-Cells-Meet-Keratin.html |

|
|
|
|
|